Department of Otorhinolaryngology, University Medical Center Hamburg-Eppendorf, Martinistraße 52, 20246, Hamburg, Germany.
Clinical Cancer Registry, University Cancer Center Hamburg, University Medical Center Hamburg-Eppendorf, Martinistraße 52, 20246, Hamburg, Germany.
J Cancer Res Clin Oncol. 2021 Feb;147(2):549-559. doi: 10.1007/s00432-020-03352-1. Epub 2020 Aug 18.
Controversies exist in regard to surgical neck management in total laryngectomies (TL). International guidelines do not sufficiently discriminate neck sides and sublevels, or minimal neck-dissection nodal yield (NY).
Thirty-seven consecutive primary TL cases from 2009 to 2019 were retrospectively analyzed in terms of local tumor growth using a previously established imaging scheme, metastatic neck involvement, and NY impact on survival.
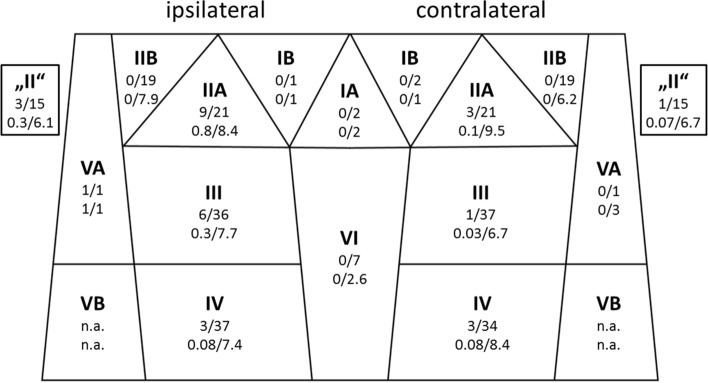
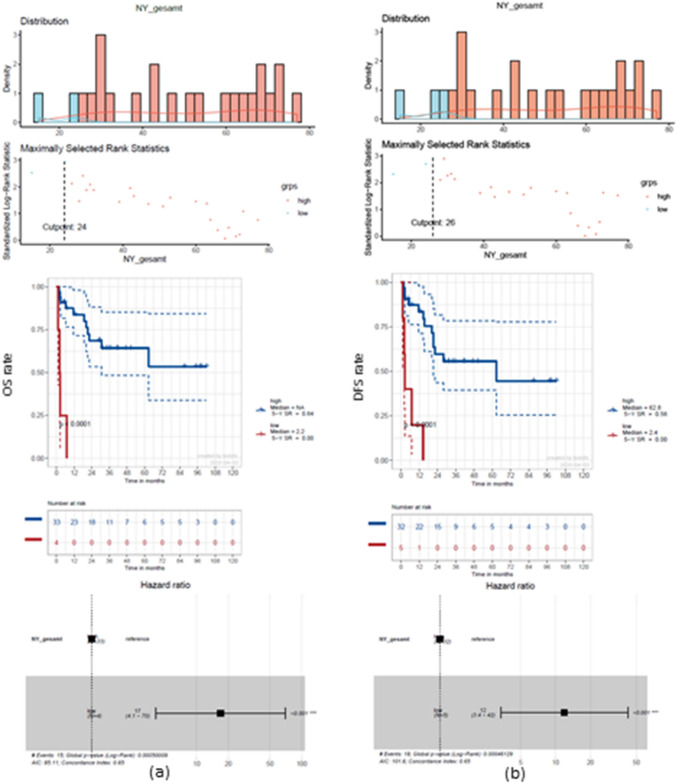
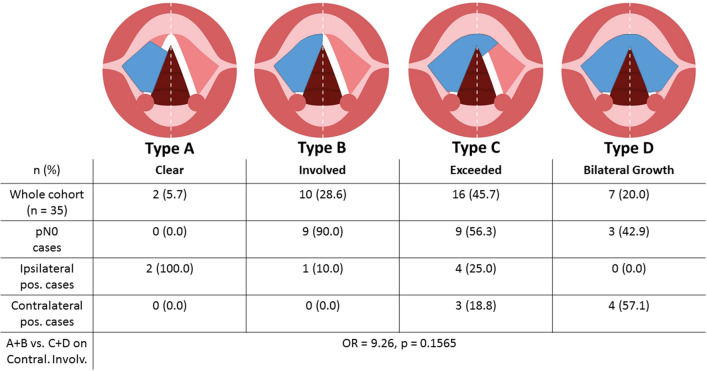
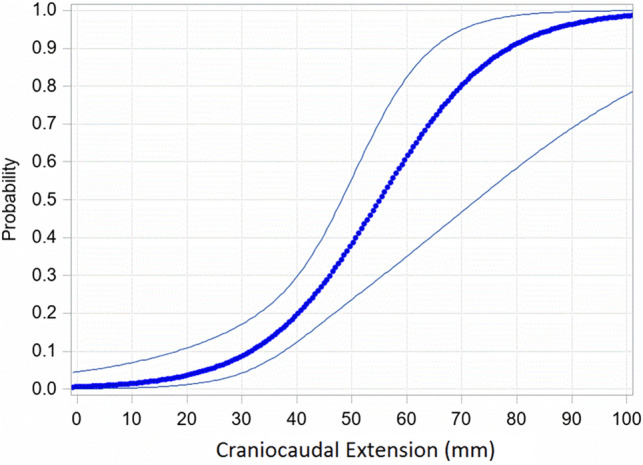
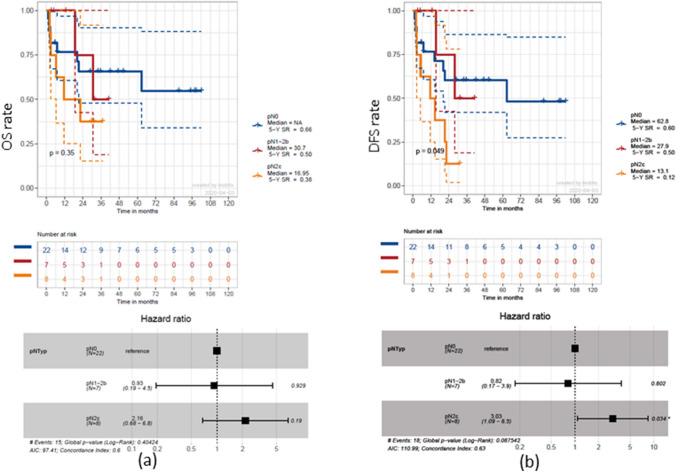
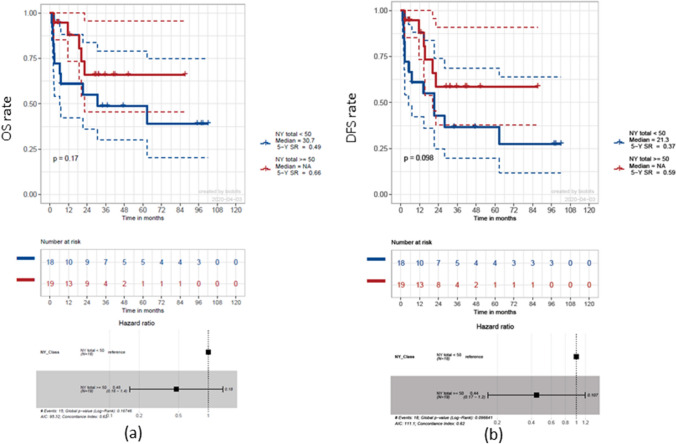
There was no case of level IIB involvement on any side. For type A and B tumor midline involvement, no positive contralateral lymph nodes were found. Craniocaudal tumor extension correlated with contralateral neck involvement (OR: 1.098, p = 0.0493) and showed increased involvement when extending 33 mm (p = 0.0134). Using a bilateral NY of ≥ 24 for 5-year overall survival (OS) and ≥ 26 for 5-year disease-free survival (DFS) gave significantly increased rate advantages of 64 and 56%, respectively (both p < 0.0001).
This work sheds light on regional metastatic distribution pattern and its influence on TL cases. An NY of n ≥ 26 can be considered a desirable benchmark for bilateral selective neck dissections as it leads to improved OS and DFS. Therefore, an omission of distinct neck levels cannot be promoted at this time.
全喉切除术(TL)中外科颈管理存在争议。国际指南没有充分区分颈部侧区和亚区,或最小颈部解剖淋巴结产量(NY)。
回顾性分析了 2009 年至 2019 年连续 37 例原发性 TL 病例,根据之前建立的影像学方案评估局部肿瘤生长、转移性颈部受累情况以及 NY 对生存的影响。
任何一侧均无 IIB 级受累病例。对于 A 型和 B 型肿瘤中线受累,未发现对侧淋巴结阳性。头侧-尾侧肿瘤延伸与对侧颈部受累相关(OR:1.098,p=0.0493),当延伸 33mm 时,受累增加(p=0.0134)。对于 5 年总生存率(OS)为双侧 NY≥24,5 年无病生存率(DFS)为双侧 NY≥26,分别显著提高了 64%和 56%的优势率(均 p<0.0001)。
这项工作揭示了区域转移性分布模式及其对 TL 病例的影响。NY≥26 可被视为双侧选择性颈部清扫术的理想基准,因为它可提高 OS 和 DFS。因此,目前不能提倡省略特定的颈部水平。