Eastern Regional Emergency Healthcare Network, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands.
Department of Emergency Medicine, Radboud University Medical Center, Nijmegen, The Netherlands.
BMC Fam Pract. 2020 Aug 20;21(1):171. doi: 10.1186/s12875-020-01220-y.
In the Netherlands, community-dwelling older people with primary care emergency problems contact the General Practitioner Cooperative (GPC) after hours. However, frailty remains an often unobserved hazard with adverse health outcomes. The aim of this study was to provide insight into differences between older persons with or without GPC emergency care visits (reference group) regarding frailty and healthcare use.
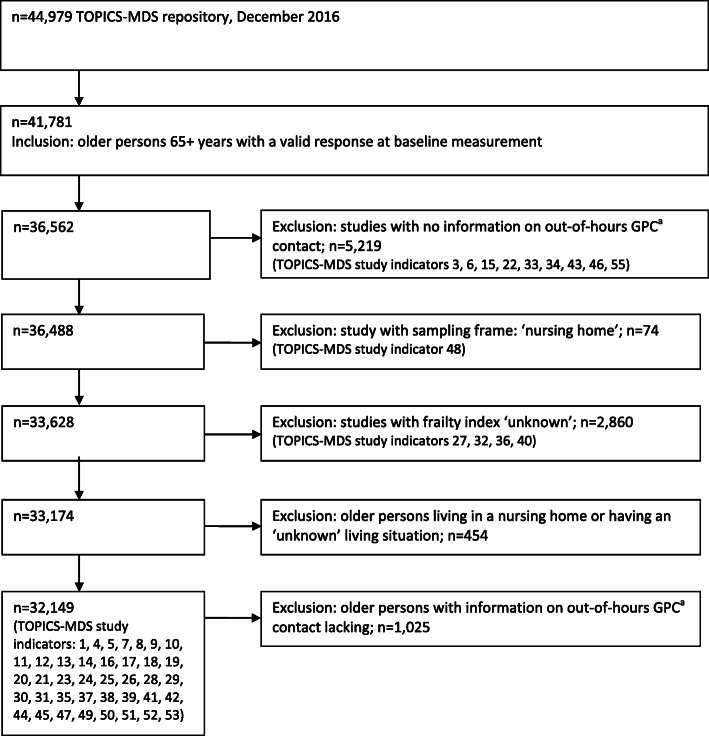
A cross-sectional descriptive study design was based on data from the public data repository of The Older Persons and Informal Caregivers Survey Minimum Dataset (TOPICS-MDS). Frailty in older persons (65+ years, n = 32,149) was measured by comorbidity, functional and psychosocial aspects, quality of life and a frailty index. Furthermore, home care use and hospital admissions of older persons were identified. We performed multilevel logistic and linear regression analyses. A random intercept model was utilised to test differences between groups, and adjustment factors (confounders) were used in the multilevel analysis.
Compared to the reference group, older persons with GPC contact were frailer in the domain of comorbidity (mean difference 0.52; 95% CI 0.47-0.57, p < 0.0001) and functional limitations (mean difference 0.53; 95% CI 0.46-0.60, p < 0.0001), and they reported less emotional wellbeing (mean difference - 4.10; 95% CI -4.59- -3.60, p < 0.0001) and experienced a lower quality of life (mean difference - 0.057; 95% CI -0.064- -0.050, p < 0.0001). Moreover, older persons more often reported limited social functioning (OR = 1.50; 95% CI 1.39-1.62, p < 0.0001) and limited perceived health (OR = 1.50, 95% CI 1.39-1.62, p < 0.0001). Finally, older persons with GPC contact more often used home care (OR = 1.37; 95% CI 1.28-1.47, p < 0.0001) or were more often admitted to the hospital (OR = 2.88; 95% CI 2.71-3.06, p < 0.0001).
Older persons with out-of-hours GPC contact for an emergency care visit were significantly frailer in all domains and more likely to use home care or to be admitted to the hospital compared to the reference group. Potentially frail older persons seemed to require adequate identification of frailty and support (e.g., advanced care planning) both before and after a contact with the out-of-hours GPC.
在荷兰,有初级保健急诊问题的社区居住的老年人在非工作时间会联系全科医生合作组织(GPC)。然而,脆弱仍然是一个经常未被发现的危险,会导致不良的健康后果。本研究的目的是了解有或没有 GPC 急诊就诊的老年人(参照组)在脆弱和医疗保健使用方面的差异。
本研究采用了横断面描述性研究设计,数据来自公共数据存储库中的老年人和非正式护理者调查最小数据集(TOPICS-MDS)。使用共病、功能和心理社会方面、生活质量和脆弱指数来衡量老年人的脆弱程度(65 岁以上,n=32149)。还确定了老年人的家庭护理使用情况和住院情况。我们进行了多水平逻辑和线性回归分析。使用随机截距模型来检验组间差异,并在多水平分析中使用调整因素(混杂因素)。
与参照组相比,有 GPC 联系的老年人在共病(平均差异 0.52;95%置信区间 0.47-0.57,p<0.0001)和功能障碍(平均差异 0.53;95%置信区间 0.46-0.60,p<0.0001)方面更为脆弱,他们报告的情绪健康状况较差(平均差异-4.10;95%置信区间-4.59- -3.60,p<0.0001)和生活质量较低(平均差异-0.057;95%置信区间-0.064- -0.050,p<0.0001)。此外,老年人更经常报告社交功能受限(优势比 OR=1.50;95%置信区间 1.39-1.62,p<0.0001)和感知健康受限(OR=1.50,95%置信区间 1.39-1.62,p<0.0001)。最后,有 GPC 联系的老年人更经常使用家庭护理(优势比 OR=1.37;95%置信区间 1.28-1.47,p<0.0001)或更经常住院(优势比 OR=2.88;95%置信区间 2.71-3.06,p<0.0001)。
与参照组相比,在非工作时间因急诊就诊而联系 GPC 的老年人在所有领域都明显更为脆弱,并且更有可能使用家庭护理或住院治疗。潜在的脆弱老年人在与非工作时间 GPC 联系之前和之后似乎都需要充分识别脆弱性并提供支持(例如,预先护理计划)。