Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, USA.
Department of Data Sciences, Dana-Farber Cancer Institute, Boston, MA, USA.
Leukemia. 2021 Apr;35(4):1064-1072. doi: 10.1038/s41375-020-01010-6. Epub 2020 Aug 20.
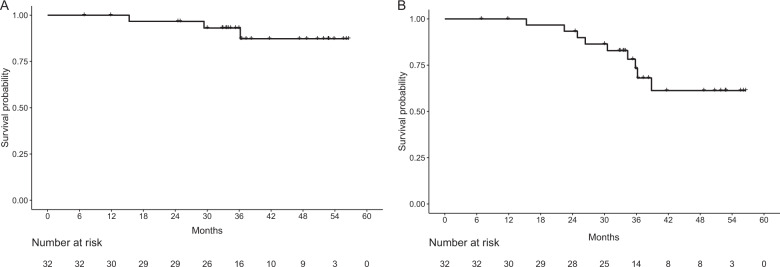
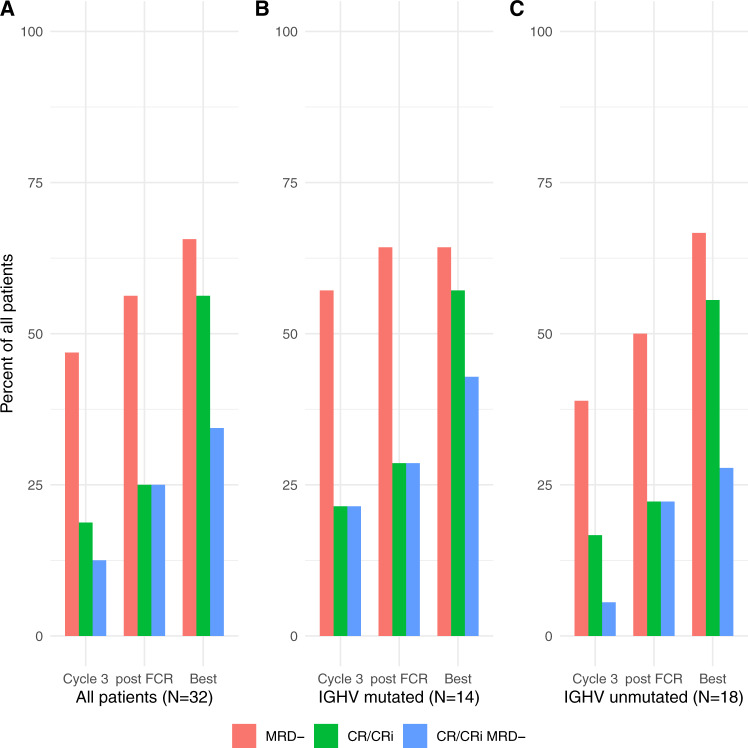
Fludarabine, cyclophosphamide, and rituximab (FCR) is highly effective initial therapy for younger patients with chronic lymphocytic leukemia (CLL); however, most eventually relapse. Duvelisib is a delta/gamma PI3K inhibitor approved for relapsed/refractory CLL. We conducted an investigator-initiated, phase 1b/2 study of duvelisib + FCR (DFCR) as initial treatment for CLL patients aged ≤65. A standard 3 + 3 design included two dose levels of duvelisib (25 mg qd and 25 mg bid). Duvelisib was given for 1 week, then with standard FCR added for up to six 28-day cycles, then up to 2 years of duvelisib maintenance. Thirty-two patients were enrolled. The phase 2 dose of duvelisib was identified as 25 mg bid. Hematologic toxicity was common, and all-grade non-hematologic toxicities included transaminitis (28%), febrile neutropenia (22%), pneumonia (19%), and colitis (6%). The best overall response rate by ITT was 88% (56% CR/CRi and 32% PR). The best rate of bone marrow undetectable minimal residual disease (BM-uMRD) by ITT was 66%. The rate of CR with BM-uMRD at end of combination treatment (primary endpoint) was 25%. Three-year PFS and OS are 73 and 93%, respectively. DFCR is active as initial therapy of younger CLL patients. Immune-mediated and infectious toxicities occurred and required active management.
氟达拉滨、环磷酰胺和利妥昔单抗(FCR)是年轻慢性淋巴细胞白血病(CLL)患者的有效初始治疗方法;然而,大多数患者最终会复发。Duvelisib 是一种已批准用于治疗复发/难治性 CLL 的 δ/gamma PI3K 抑制剂。我们开展了一项由研究者发起的、评估 Duvelisib+FCR(DFCR)作为 ≤65 岁 CLL 患者初始治疗的 1b/2 期研究。该研究采用标准的 3+3 设计,包括 Duvelisib 的两个剂量水平(25mg qd 和 25mg bid)。Duvelisib 治疗 1 周,随后加入标准的 FCR,最多进行 6 个 28 天周期的治疗,随后最多进行 2 年的 Duvelisib 维持治疗。共纳入 32 例患者。Duvelisib 的 2 期剂量确定为 25mg bid。血液学毒性常见,所有级别非血液学毒性包括转氨基酶升高(28%)、发热性中性粒细胞减少症(22%)、肺炎(19%)和结肠炎(6%)。按意向治疗(ITT)评估的最佳总缓解率为 88%(56%完全缓解/伴有不完全血液学恢复的完全缓解和 32%部分缓解)。按 ITT 评估的骨髓不可检测微小残留病(BM-uMRD)最佳缓解率为 66%。联合治疗结束时(主要终点)达到完全缓解且伴有 BM-uMRD 的比例为 25%。3 年无进展生存(PFS)率和总生存(OS)率分别为 73%和 93%。DFCR 是年轻 CLL 患者的有效初始治疗方法。免疫介导和感染毒性发生,需要积极管理。