Cedars-Sinai Medical Center, Smidt Heart Institute, Los Angeles, CA, USA.
Department of Cardiovascular Medicine, First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, Shaanxi, China.
J Physiol. 2020 Nov;598(22):5091-5108. doi: 10.1113/JP280425. Epub 2020 Sep 9.
Heart failure (HF), the leading cause of death in developed countries, occurs in the setting of reduced (HFrEF) or preserved (HFpEF) ejection fraction. Unlike HFrEF, there are no effective treatments for HFpEF, which accounts for ∼50% of heart failure. Abnormal intracellular calcium dynamics in cardiomyocytes have major implications for contractility and rhythm, but compared to HFrEF, very little is known about calcium cycling in HFpEF. We used rat models of HFpEF and HFrEF to reveal distinct differences in intracellular calcium regulation and excitation-contraction (EC) coupling. While HFrEF is characterized by defective EC coupling at baseline, HFpEF exhibits enhanced coupling fidelity, further aggravated by a reduction in β-adrenergic sensitivity. These differences in EC coupling and β-adrenergic sensitivity may help explain why therapies that work in HFrEF are ineffective in HFpEF.
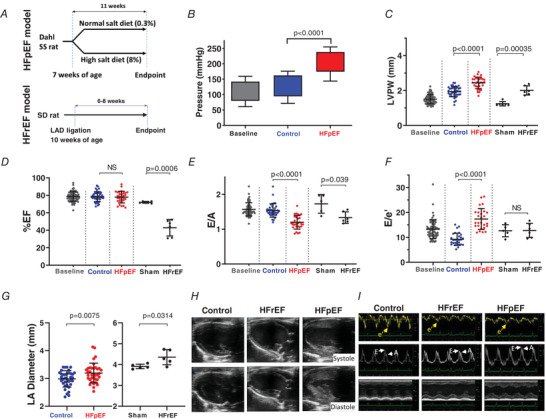
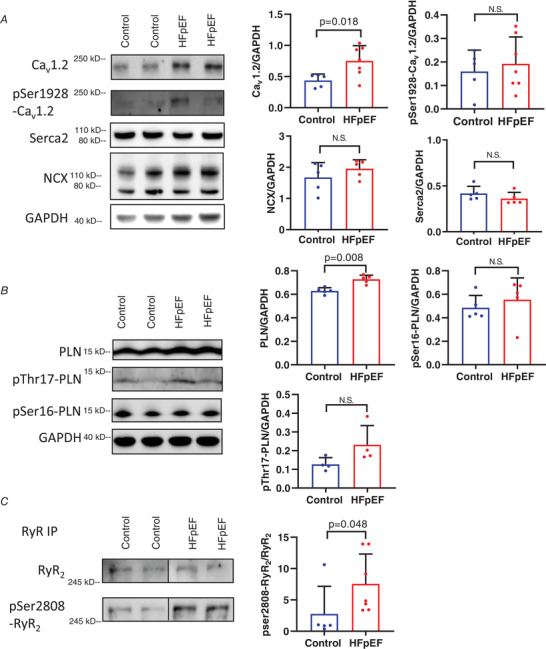
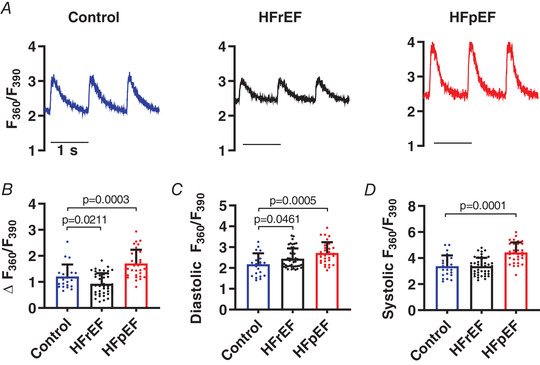
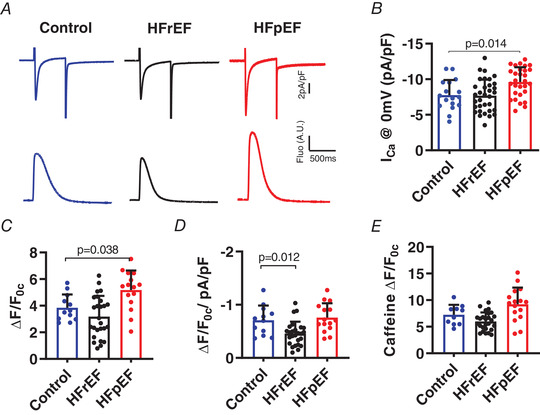
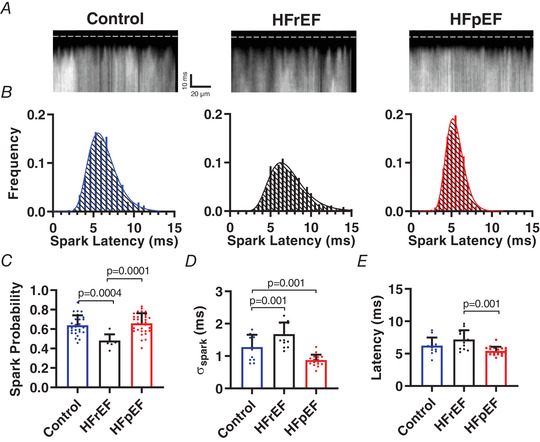
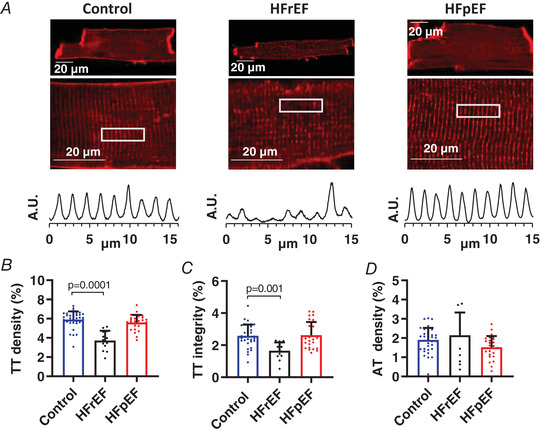
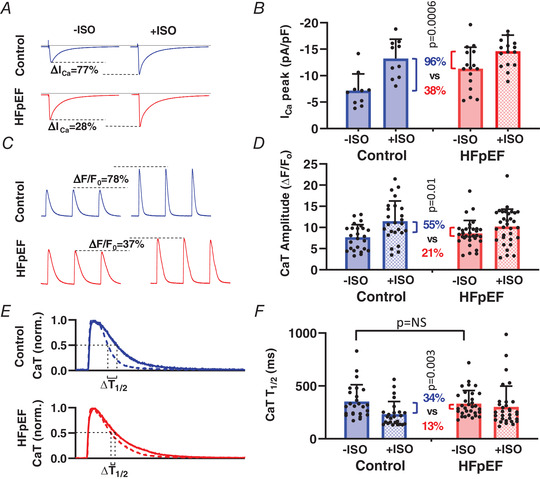
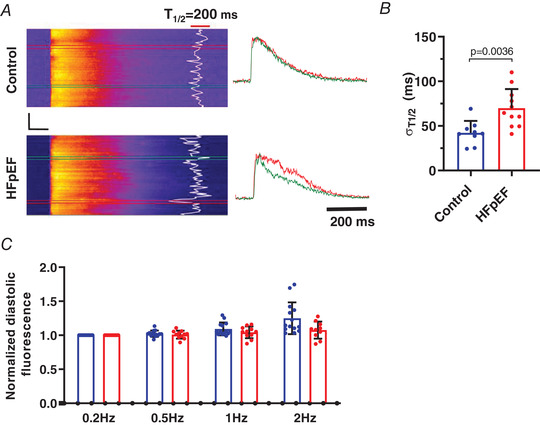
Heart failure with reduced or preserved ejection fraction (respectively, HFrEF and HFpEF) is the leading cause of death in developed countries. Although numerous therapies improve outcomes in HFrEF, there are no effective treatments for HFpEF. We studied phenotypically verified rat models of HFrEF and HFpEF to compare excitation-contraction (EC) coupling and protein expression in these two forms of heart failure. Dahl salt-sensitive rats were fed a high-salt diet (8% NaCl) from 7 weeks of age to induce HFpEF. Impaired diastolic relaxation and preserved ejection fraction were confirmed in each animal echocardiographically, and clinical signs of heart failure were documented. To generate HFrEF, Sprague-Dawley (SD) rats underwent permanent left anterior descending coronary artery ligation which, 8-10 weeks later, led to systolic dysfunction (verified echocardiographically) and clinical signs of heart failure. Calcium (Ca ) transients were measured in isolated cardiomyocytes under field stimulation or patch clamp. Ultra-high-speed laser scanning confocal imaging captured Ca sparks evoked by voltage steps. Western blotting and PCR were used to assay changes in EC coupling protein and RNA expression. Cardiomyocytes from rats with HFrEF exhibited impaired EC coupling, including decreased Ca transient (CaT) amplitude and defective couplon recruitment, associated with transverse (t)-tubule disruption. In stark contrast, HFpEF cardiomyocytes showed saturated EC coupling (increased I , high probability of couplon recruitment with greater Ca release synchrony, increased CaT) and preserved t-tubule integrity. β-Adrenergic stimulation of HFpEF myocytes with isoprenaline (isoproterenol) failed to elicit robust increases in I or CaT and relaxation kinetics. Fundamental differences in EC coupling distinguish HFrEF from HFpEF.
心力衰竭(HF)是发达国家的主要死亡原因,发生在射血分数降低(HFrEF)或保留(HFpEF)的情况下。与 HFrEF 不同,HFpEF 尚无有效治疗方法,约占心力衰竭的 50%。心肌细胞内钙离子动力学异常对收缩性和节律有重大影响,但与 HFrEF 相比,HFpEF 中的钙离子循环知之甚少。我们使用 HFpEF 和 HFrEF 的大鼠模型揭示了细胞内钙调节和兴奋-收缩(EC)偶联的明显差异。虽然 HFrEF 的特征是基线时 EC 偶联有缺陷,但 HFpEF 表现出增强的偶联保真度,β-肾上腺素能敏感性降低进一步加重了这种情况。这些 EC 偶联和 β-肾上腺素能敏感性的差异可能有助于解释为什么在 HFrEF 中有效的治疗方法在 HFpEF 中无效。
射血分数降低或保留的心力衰竭(分别为 HFrEF 和 HFpEF)是发达国家的主要死亡原因。尽管有许多疗法可改善 HFrEF 的预后,但 HFpEF 尚无有效治疗方法。我们研究了表型验证的 HFrEF 和 HFpEF 大鼠模型,以比较这两种心力衰竭形式的 EC 偶联和蛋白表达。从 7 周龄开始,用高盐饮食(8%NaCl)喂养 Dahl 盐敏感大鼠以诱导 HFpEF。每只动物的超声心动图均证实舒张功能障碍和射血分数保留,并记录心力衰竭的临床症状。为了产生 HFrEF,Sprague-Dawley(SD)大鼠接受了永久性左前降支冠状动脉结扎术,8-10 周后导致收缩功能障碍(超声心动图证实)和心力衰竭的临床症状。在离体心肌细胞中,通过场刺激或膜片钳测量钙瞬变。超高速度激光扫描共聚焦成像捕获由电压阶跃引起的 Ca 火花。使用 Western blot 和 PCR 检测 EC 偶联蛋白和 RNA 表达的变化。HFrEF 大鼠的心肌细胞表现出 EC 偶联受损,包括 Ca 瞬变(CaT)幅度降低和偶联子募集缺陷,与横(t)小管破坏有关。相比之下,HFpEF 心肌细胞显示出饱和的 EC 偶联(I 增加,偶联子募集的高概率和更大的 Ca 释放同步性,CaT 增加)和保留 t-小管完整性。HFpEF 心肌细胞用异丙肾上腺素(isoproterenol)刺激β-肾上腺素能,未能引起 I 或 CaT 和松弛动力学的显著增加。EC 偶联的根本差异将 HFrEF 与 HFpEF 区分开来。