Centre for Trials Research, Cardiff University, 4th Floor, Neuadd Meirionnydd, Heath Park, Cardiff, CF14 4YS, UK.
School of Optometry and Vision Sciences, College of Biomedical and Life Sciences, Cardiff University, Maindy Road, Cardiff, CF24 4HQ, UK.
BMC Psychiatry. 2020 Aug 26;20(1):419. doi: 10.1186/s12888-020-02805-8.
Undetected depression is common in people with low vision and depression screening has been recommended. However, depression screening is a complex procedure for which low vision practitioners need training. This study examined the integration of routine depression screening, using two questions, and referral pathways into a national low vision service in Wales at 6 months following practitioner training, and identified key barriers to implementation.
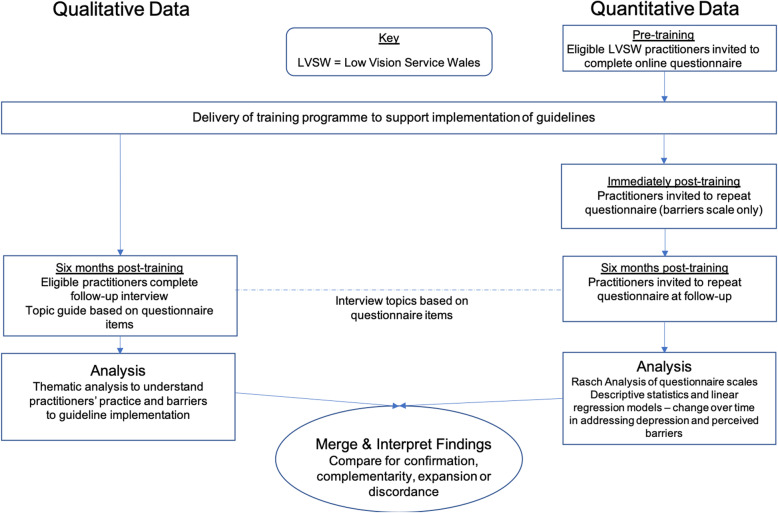
This pre-post single group study employed a convergent mixed methods design to collect quantitative questionnaire and qualitative interview data on low vision practitioners' clinical practice and perceived barriers to implementing depression screening. Forty practitioners completed questionnaires pre-, immediately post- and 6 months post-training and nine engaged in interviews 6 months post-training. Ordinal questionnaire scores were Rasch-transformed into interval-level data before linear regression analyses were performed to determine the change in scores over time and the association between perceived barriers and clinical practice. Thematic Analysis was applied to the interviews and the narrative results merged with the questionnaire findings.
Before training, only one third of practitioners (n = 15) identified depression in low vision patients, increasing to over 90% (n = 37) at 6 months post-training, with a corresponding increase in those using validated depression screening questions from 10% (n = 4) to 80% (n = 32). Six months post-training, practitioners reported taking significantly more action in response to suspected depression (difference in means = 2.77, 95% CI 1.93 to 3.61, p < 0.001) and perceived less barriers to addressing depression (difference in means = - 0.95, 95% CI - 1.32 to - 0.59, p < 0.001). However, the screening questions were not used consistently. Some barriers to implementation remained, including perceived patient reluctance to discuss depression, time constraints and lack of confidence in addressing depression.
The introduction of depression screening service guidelines and training successfully increased the number of low vision practitioners identifying and addressing depression. However, standardized screening of all low vision attendees has not yet been achieved and several barriers remain. Healthcare services need to address these barriers when considering mental health screening, and further research could focus on the process from the patients' perspective, to determine the desire for and acceptability of screening.
视力低下人群中普遍存在未被发现的抑郁症,因此建议进行抑郁筛查。然而,对于视力低下从业者来说,抑郁筛查是一个复杂的过程,他们需要接受培训。本研究在对从业者进行培训 6 个月后,调查了将使用两个问题进行常规抑郁筛查和转诊途径纳入威尔士国家低视力服务的情况,并确定了实施过程中的关键障碍。
本项预-后单组研究采用收敛混合方法设计,收集了低视力从业者临床实践和实施抑郁筛查的感知障碍的定量问卷和定性访谈数据。40 名从业者在培训前、培训后立即和培训后 6 个月完成了问卷,9 人在培训后 6 个月进行了访谈。对问卷得分进行了 RAST 转换,将其转换为区间水平数据,然后进行线性回归分析,以确定随时间的得分变化以及感知障碍与临床实践之间的关系。对访谈进行了主题分析,并将叙事结果与问卷结果合并。
培训前,只有三分之一的从业者(n=15)能在低视力患者中识别抑郁症,培训后 6 个月增加到 90%以上(n=37),同时使用经过验证的抑郁筛查问题的从业者从 10%(n=4)增加到 80%(n=32)。培训后 6 个月,从业者报告称在疑似抑郁症方面采取了更多行动(平均差异=2.77,95%置信区间为 1.93 至 3.61,p<0.001),且认为解决抑郁症的障碍较少(平均差异=-0.95,95%置信区间为-1.32 至-0.59,p<0.001)。然而,这些筛查问题并未得到一致使用。实施仍存在一些障碍,包括患者不愿讨论抑郁、时间限制以及对处理抑郁缺乏信心。
引入抑郁筛查服务指南和培训成功增加了识别和处理抑郁症的低视力从业者数量。然而,尚未实现对所有低视力就诊者进行标准化筛查,仍存在一些障碍。医疗保健服务在考虑进行心理健康筛查时需要解决这些障碍,进一步的研究可以从患者的角度关注筛查的需求和可接受性。