Lan Nan, Hull Tracy L, Shen Bo
Center for Inflammatory Bowel Disease, Digestive Disease and Surgery Institute, Cleveland Clinic, Cleveland, OH, USA.
Center for Inflammatory Bowel Diseases, Columbia University Irving Medical Center-New York Presbyterian Hospital, New York, NY 10032, USA. Fax. 1 212 305 0267. Email:
Gastroenterol Rep (Oxf). 2020 Feb 5;8(4):312-318. doi: 10.1093/gastro/goz071. eCollection 2020 Aug.
Stricture is a common presentation of Crohn's disease with the site of prevalence being the distal ileum. This study aimed to compare the efficacy and safety of patients with primary distal ileum stricture treated with endoscopic stricturotomy (ESt) vs ileo-colonic resection (ICR).
All consecutive patients with primary distal ileum stricture that were treated with ESt and/or ICR were extracted from the interventional inflammatory bowel disease (-IBD) unit from 2001 to 2016. All patients with a stricture >5 cm or those with anastomotic strictures were excluded from the study. The primary outcomes were surgery-free survival and post-procedural complications.
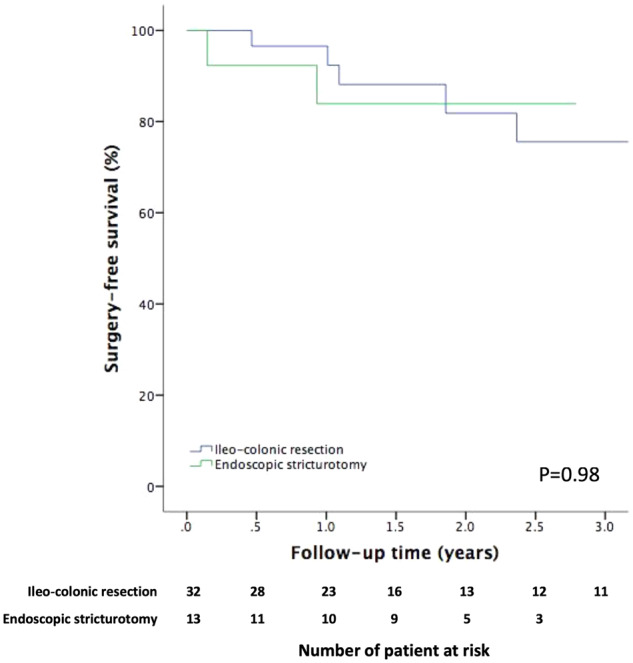
A total of 13 patients receiving ESt and 32 patients receiving ICR were included in this study. Although the length of the stricture is comparable between the two groups (2.4 ± 0.9 vs 3.0 ± 1.1 cm, =0.17), patients who received surgery had a more complicated obstruction presented by the high pre-stenosis proximal dilation rate (67.7% vs 9.1%, =0.001). All patients in both groups achieved immediate technical success after treatment. The median follow-up durations were 1.8 and 1.5 years in the ESt and ICR groups, respectively. The subsequent surgery rates were similar between the two groups (15.4% vs 18.8%, =0.79) and the overall surgery-free survival was also comparable between the two groups (=0.98). Post-procedural adverse events were seen in 2/29 ESt procedures (6.9% per procedure) and 8/32 (25.0%) patients receiving ICR (=0.05).
ESt achieved comparable stricture-related surgery-free survival as ICR, while ESt had a numerically lower post-operative complication rate.
狭窄是克罗恩病的常见表现,好发部位为回肠末端。本研究旨在比较内镜下狭窄切开术(ESt)与回结肠切除术(ICR)治疗原发性回肠末端狭窄患者的疗效和安全性。
从2001年至2016年介入性炎症性肠病(-IBD)科室中提取所有接受ESt和/或ICR治疗的原发性回肠末端狭窄的连续患者。所有狭窄长度>5 cm或吻合口狭窄的患者均被排除在研究之外。主要结局为无手术生存期和术后并发症。
本研究共纳入13例接受ESt治疗的患者和32例接受ICR治疗的患者。尽管两组狭窄长度相当(2.4±0.9 vs 3.0±1.1 cm,P = 0.17),但接受手术治疗的患者梗阻情况更为复杂,狭窄近端扩张率较高(67.7% vs 9.1%,P = 0.001)。两组所有患者治疗后均立即取得技术成功。ESt组和ICR组的中位随访时间分别为1.8年和1.5年。两组随后的手术率相似(15.4% vs 18.8%,P = 0.79),总体无手术生存期也相当(P = 0.98)。2/29例ESt手术(每例手术6.9%)和8/32例(25.0%)接受ICR治疗的患者出现术后不良事件(P = 0.05)。
ESt与ICR在无狭窄相关手术生存期方面相当,而ESt术后并发症发生率在数值上较低。