Department of Infectious Diseases, Shanghai Children's Medical Center, Shanghai Jiaotong University School of Medicine, Shanghai, China.
The Laboratory of Pediatric Infectious Diseases, Pediatric Translational Medicine Institute, Shanghai Children's Medical Center, Shanghai Jiaotong University School of Medicine, Shanghai, China.
BMC Infect Dis. 2020 Aug 26;20(1):633. doi: 10.1186/s12879-020-05356-1.
Cases of refractory Mycoplasma pneumoniae pneumonia have been increasing recently; however, whether viral coinfection or macrolide-resistant M. infection contribute to the development of refractory M. pneumoniae pneumonia remains unclear. This study aimed to investigate the impacts of viral coinfection and macrolide-resistant M. pneumoniae infection on M. pneumoniae pneumonia in hospitalized children and build a model to predict a severe disease course.
Nasopharyngeal swabs or sputum specimens were collected from patients with community-acquired pneumonia meeting our protocol who were admitted to Shanghai Children's Medical Center from December 1, 2016, to May 31, 2019. The specimens were tested with the FilmArray Respiratory Panel, a multiplex polymerase chain reaction assay that detects 16 viruses, Bordetella pertussis, M. pneumoniae, and Chlamydophila pneumoniae. Univariate and multivariate logistic regression models were used to identify the risk factors for adenovirus coinfection and macrolide-resistant mycoplasma infection.
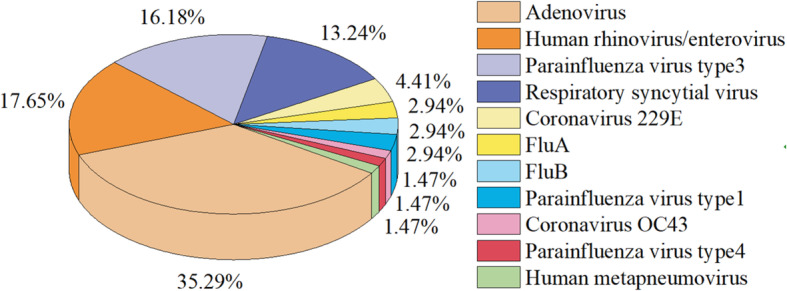
Among the 107 M. pneumoniae pneumonia patients, the coinfection rate was 56.07%, and 60 (60/107, 56.07%) patients were infected by drug-resistant M. pneumoniae. Adenovirus was the most prevalent coinfecting organism, accounting for 22.43% (24/107). The classification tree confirmed that viral coinfection was more common in patients younger than 3 years old. Adenovirus coinfection and drug-resistant M. pneumoniae infection occurred more commonly in patients with refractory M. pneumoniae pneumonia (P = 0.019; P = 0.001). A prediction model including wheezing, lung consolidation and extrapulmonary complications was used to predict adenovirus coinfection. The area under the receiver operating characteristic curve of the prediction model was 0.795 (95% CI 0.679-0.893, P < 0.001). A prolonged fever duration after the application of macrolides for 48 h was found more commonly in patients infected by drug-resistant M. pneumoniae (P = 0.002). A fever duration longer than 7 days was an independent risk factor for drug-resistant Mycoplasma infection (OR = 3.500, 95% CI = 1.310-9.353, P = 0.012).
The occurrence of refractory M. pneumoniae pneumonia is associated with adenovirus coinfection and infection by drug-resistant M. pneumoniae. A prediction model combining wheezing, extrapulmonary complications and lung consolidation can be used to predict adenovirus coinfection in children with M. pneumoniae pneumonia. A prolonged fever duration indicates drug-resistant M. pneumoniae infection, and a reasonable change in antibiotics is necessary.
最近,耐甲氧西林肺炎支原体肺炎的病例一直在增加;然而,病毒合并感染或耐大环内酯类肺炎支原体感染是否会导致难治性肺炎支原体肺炎的发生尚不清楚。本研究旨在探讨病毒合并感染和耐大环内酯类肺炎支原体感染对住院儿童肺炎支原体肺炎的影响,并建立预测严重疾病过程的模型。
收集 2016 年 12 月 1 日至 2019 年 5 月 31 日因社区获得性肺炎入住上海儿童医学中心的患者的鼻咽拭子或痰标本,这些患者符合我们的方案。采用 FilmArray 呼吸道面板进行检测,该多重聚合酶链反应检测 16 种病毒、百日咳博德特氏菌、肺炎支原体和肺炎衣原体。采用单因素和多因素逻辑回归模型来确定腺病毒合并感染和耐大环内酯类肺炎支原体感染的危险因素。
在 107 例肺炎支原体肺炎患者中,合并感染率为 56.07%,60 例(60/107,56.07%)患者感染耐大环内酯类肺炎支原体。腺病毒是最常见的合并感染病原体,占 22.43%(24/107)。分类树证实,病毒合并感染在 3 岁以下的患者中更为常见。腺病毒合并感染和耐大环内酯类肺炎支原体感染在难治性肺炎支原体肺炎患者中更为常见(P=0.019;P=0.001)。包括喘息、肺部实变和肺外并发症的预测模型用于预测腺病毒合并感染。该预测模型的受试者工作特征曲线下面积为 0.795(95%CI 0.679-0.893,P<0.001)。在应用大环内酯类药物 48 小时后,发热持续时间延长的患者更常见于耐大环内酯类肺炎支原体感染(P=0.002)。发热持续时间超过 7 天是耐肺炎支原体感染的独立危险因素(OR=3.500,95%CI=1.310-9.353,P=0.012)。
难治性肺炎支原体肺炎的发生与腺病毒合并感染和耐大环内酯类肺炎支原体感染有关。一种结合喘息、肺外并发症和肺部实变的预测模型可用于预测儿童肺炎支原体肺炎中的腺病毒合并感染。发热持续时间延长提示耐肺炎支原体感染,需要合理改变抗生素。