Department of Neurology, Affiliated Hospital of Jining Medical University, 89 Guhuai Road, Jining City, 272029, Shandong Province, China.
Medical Research Centre, Affiliated Hospital of Jining Medical University, 89 Guhuai Road, Jining City, 272029, Shandong Province, China.
BMC Neurol. 2020 Aug 26;20(1):314. doi: 10.1186/s12883-020-01895-x.
Kartagener syndrome is an autosomal recessive inherited disorder of primary ciliary dyskinesia. Moyamoya syndrome refers to a moyamoya angiopathy associated with other neurological and/or extra-neurological symptoms, or due to a well identified acquired or inherited cause. We herein reported a case of a 48-year-old woman who was favored the diagnosis of Kartagener syndrome and moyamoya syndrome. The whole genome sequencing and bioinformatics analysis showed a homozygotic nonsense mutation in the dynein, axonemal, heavy chain (DNAH) 5 gene, and heterozygotic missense mutation in the DNAH11 gene. This is the first report of the co-occurrence of the two rare diseases.
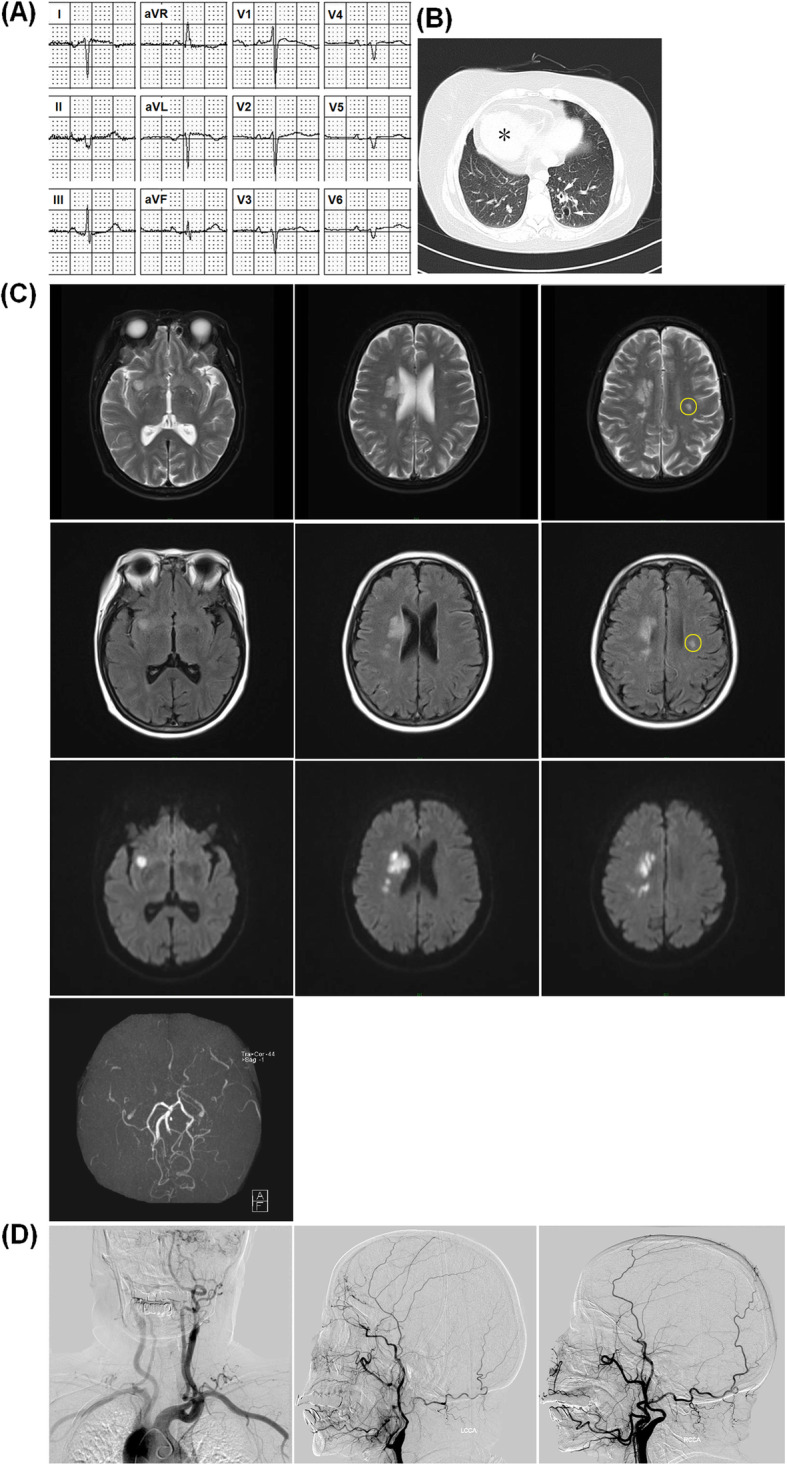
A case of a 48-year-old woman was presented with hemiplegia and slurred speech. The magnetic resonance imaging of the brain confirmed acute cerebral infarction in the right basal ganglia region, semi-oval center, insular lobe, and frontal parietal lobe. The electrocardiogram showed inverted "P" waves in L1 and AVL on left-sided chest leads and computed tomography scan of the chest showed bronchiectasis changes, cardiac shadow and apex on the right side, and situs inversus of aortic arch position. The digital subtraction angiography showed inversion of the aortic arch, and bilateral internal carotid arteries are occluded from the ophthalmic segment. The clinical, radiological, and laboratory findings made the diagnosis of Kartagener syndrome and moyamoya syndrome. The whole genome sequencing and bioinformatics analysis showed a homozygotic nonsense mutation in DNAH5 gene, and heterozygotic missense mutation in the DNAH11 gene.
The combined mutation of DNAH5 and DNAH11 may lead to the overlapping dysfunction of motile and nonmotile cilia, which contribute to the co-occurrence of Kartagener syndrome and moyamoya syndrome. Our report deserves further confirm by more case reports.
卡塔格内综合征是一种常染色体隐性遗传的原发性纤毛运动障碍疾病。烟雾病是指一种与其他神经和/或神经外症状相关的烟雾病血管病变,或由于明确的获得性或遗传性原因引起的烟雾病血管病变。本研究报道了一例 48 岁女性患者,该患者倾向于诊断为卡塔格内综合征和烟雾病。全基因组测序和生物信息学分析显示,在 dynein,axonemal,heavy chain (DNAH) 5 基因中存在纯合无义突变,在 DNAH11 基因中存在杂合错义突变。这是首例同时发生这两种罕见疾病的报道。
一名 48 岁女性患者出现偏瘫和言语不清。脑部磁共振成像证实右侧基底节区、半卵圆中心、岛叶和额顶叶有急性脑梗死。心电图显示左侧胸部导联 L1 和 AVL 导联的“P”波倒置,胸部计算机断层扫描显示支气管扩张改变,右侧心影和心尖,主动脉弓位置反转。数字减影血管造影显示主动脉弓倒置,双侧颈内动脉从眼段开始闭塞。临床、影像学和实验室检查结果提示卡塔格内综合征和烟雾病的诊断。全基因组测序和生物信息学分析显示,在 DNAH5 基因中存在纯合无义突变,在 DNAH11 基因中存在杂合错义突变。
DNAH5 和 DNAH11 的联合突变可能导致运动和非运动纤毛的重叠功能障碍,导致卡塔格内综合征和烟雾病的同时发生。我们的报告需要更多的病例报告进一步证实。