Chang Yue, Liu Qin-Yu, Zhang Qing, Rong Ya-Mei, Lu Cheng-Zhen, Li Hai
Division of Gastroenterology and Hepatology, Tianjin Xiqing Hospital, Tianjin 300380, China.
Tianjin Key Laboratory of Hepatopancreatic Fibrosis and Molecular Diagnosis and Treatment, Tianjin 300162, China.
World J Gastroenterol. 2020 Aug 7;26(29):4288-4301. doi: 10.3748/wjg.v26.i29.4288.
Hepatitis B virus-associated acute-on-chronic liver failure (HBV-ACLF) is an important type of liver failure in Asia. There is a direct relationship between HBV-ACLF and gastrointestinal barrier function. However, the nutritional status of HBV-ACLF patients has been poorly studied.
To investigate the nutritional risk and nutritional status of HBV-ACLF patients and evaluated the impact of nutritional support on the gastrointestinal barrier and 28-d mortality.
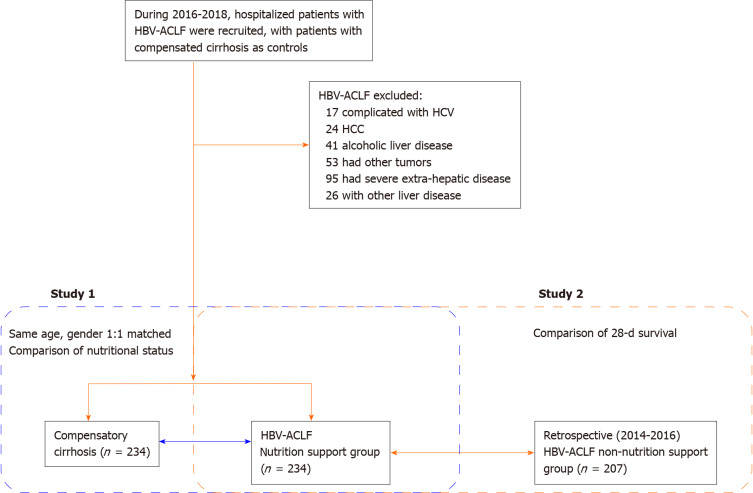
Nutritional risk screening assessment and gastrointestinal barrier biomarkers of patients with HBV-ACLF ( = 234) and patients in the compensatory period of liver cirrhosis (the control group) ( = 234) were compared during the period between 2016 and 2018. Changes were analyzed after nutritional support in HBV-ACLF patients. Valuable biomarkers have been explored to predict 28-d death. The 28-d survival between HBV-ACLF patients with nutritional support ( = 234) or no nutritional support (2014-2016) ( = 207) was compared.
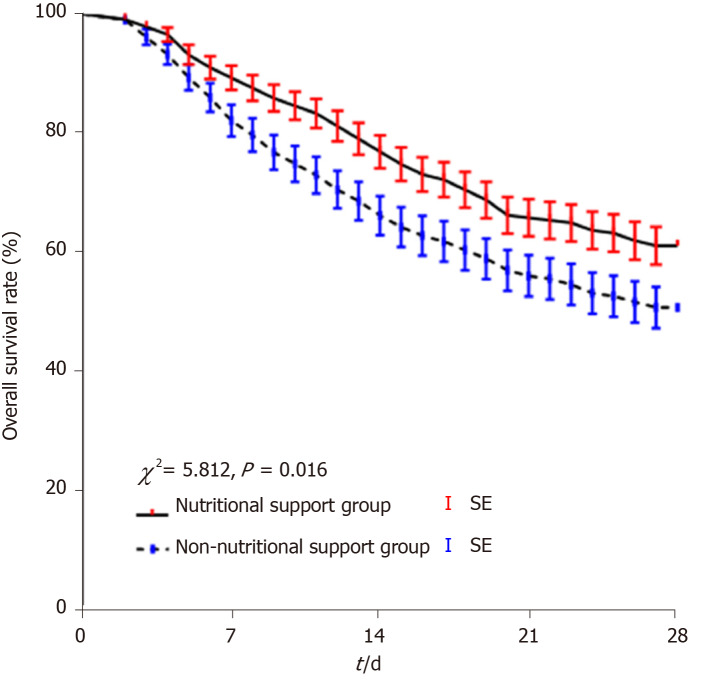
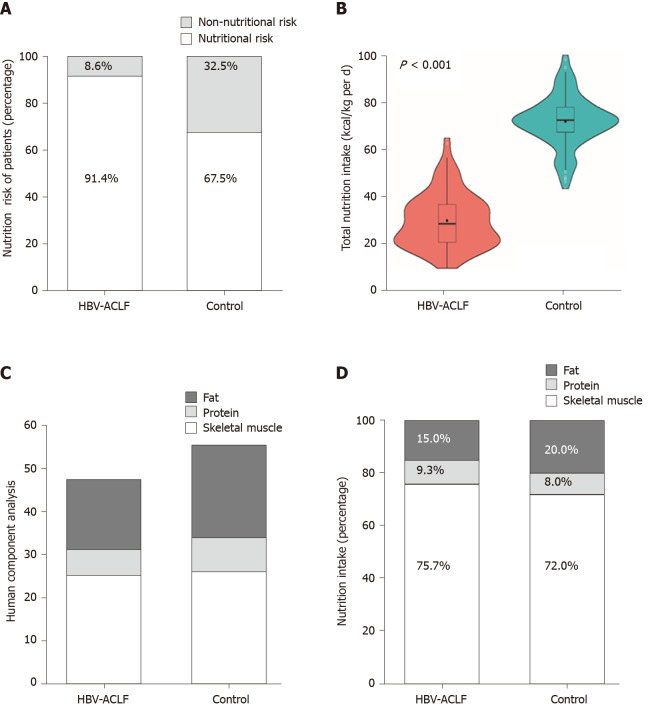
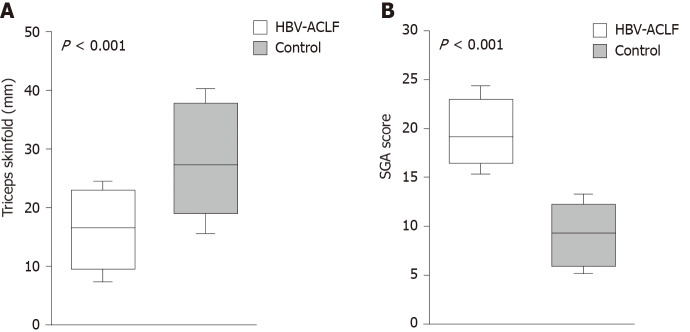
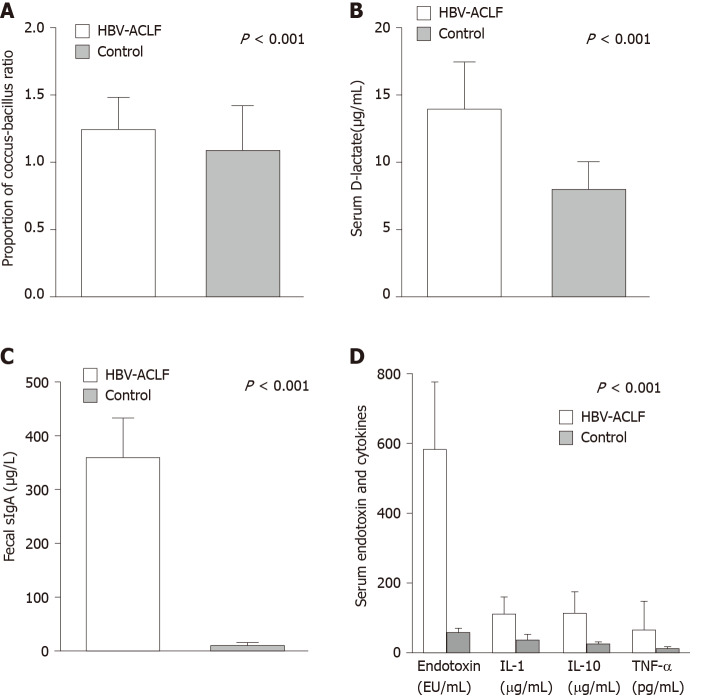
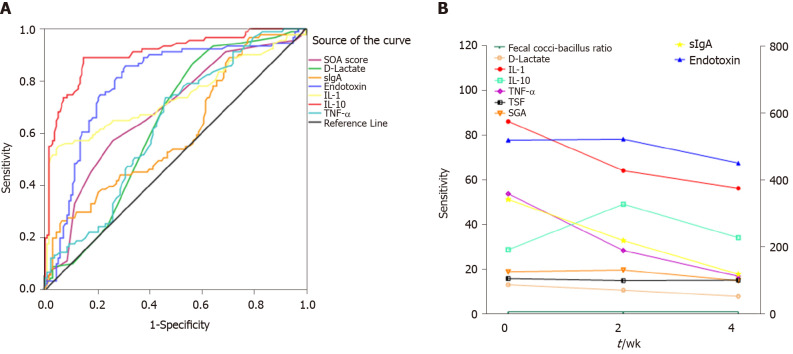
The nutritional risk of the HBV-ACLF patients was significantly higher than that of the control group. The nutritional intake of the patients with HBV-ACLF was lower than that of the control group. The decrease in skeletal muscle and fat content and the deficiency of fat intake were more obvious ( < 0.001). The coccus-bacillus ratio, secretory immunoglobulin A, and serum D-lactate were significantly increased in HBV-ACLF patients. The survival group had a lower nutritional risk, lower D-lactate, and cytokine levels (endotoxin, tumor necrosis factor alpha, interleukin-10, and interleukin-1). Interleukin-10 may be a potential predictor of death in HBV-ACLF patients. The 28-d survival of the nutritional support group was better than that of the non-nutritional support group ( = 0.016).
Patients with HBV-ACLF have insufficient nutritional intake and high nutritional risk, and their intestinal barrier function is impaired. Individualized and dynamic nutritional support is associated with a better prognosis of 28-d mortality in HBV-ACLF patients.
乙型肝炎病毒相关性慢加急性肝衰竭(HBV-ACLF)是亚洲肝衰竭的一种重要类型。HBV-ACLF与胃肠屏障功能之间存在直接关系。然而,HBV-ACLF患者的营养状况研究较少。
探讨HBV-ACLF患者的营养风险和营养状况,并评估营养支持对胃肠屏障和28天死亡率的影响。
比较2016年至2018年期间HBV-ACLF患者(n = 234)和肝硬化代偿期患者(对照组)(n = 234)的营养风险筛查评估和胃肠屏障生物标志物。分析HBV-ACLF患者营养支持后的变化。探索有价值的生物标志物以预测28天死亡率。比较接受营养支持的HBV-ACLF患者(n = 234)与未接受营养支持的患者(2014 - 2016年)(n = 207)的28天生存率。
HBV-ACLF患者的营养风险显著高于对照组。HBV-ACLF患者的营养摄入量低于对照组。骨骼肌和脂肪含量的降低以及脂肪摄入不足更为明显(P < 0.001)。HBV-ACLF患者的球菌杆菌比例、分泌型免疫球蛋白A和血清D-乳酸显著升高。存活组的营养风险、D-乳酸和细胞因子水平(内毒素、肿瘤坏死因子α、白细胞介素-10和白细胞介素-1)较低。白细胞介素-10可能是HBV-ACLF患者死亡的潜在预测指标。营养支持组的28天生存率优于非营养支持组(P = 0.016)。
HBV-ACLF患者营养摄入不足且营养风险高,其肠道屏障功能受损。个体化和动态营养支持与HBV-ACLF患者28天死亡率的较好预后相关。