Xie Lin, Chu Ran, Wang Kai, Zhang Xi, Li Jie, Zhao Zhe, Yao Shu, Wang Zhiwen, Dong Taotao, Yang Xingsheng, Su Xuantao, Qiao Xu, Song Kun, Kong Beihua
Department of Obstetrics and Gynecology, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, China.
Department of Obstetrics and Gynecology, Jining No.1 People's Hospital, Jining, China.
Front Oncol. 2020 Aug 5;10:1353. doi: 10.3389/fonc.2020.01353. eCollection 2020.
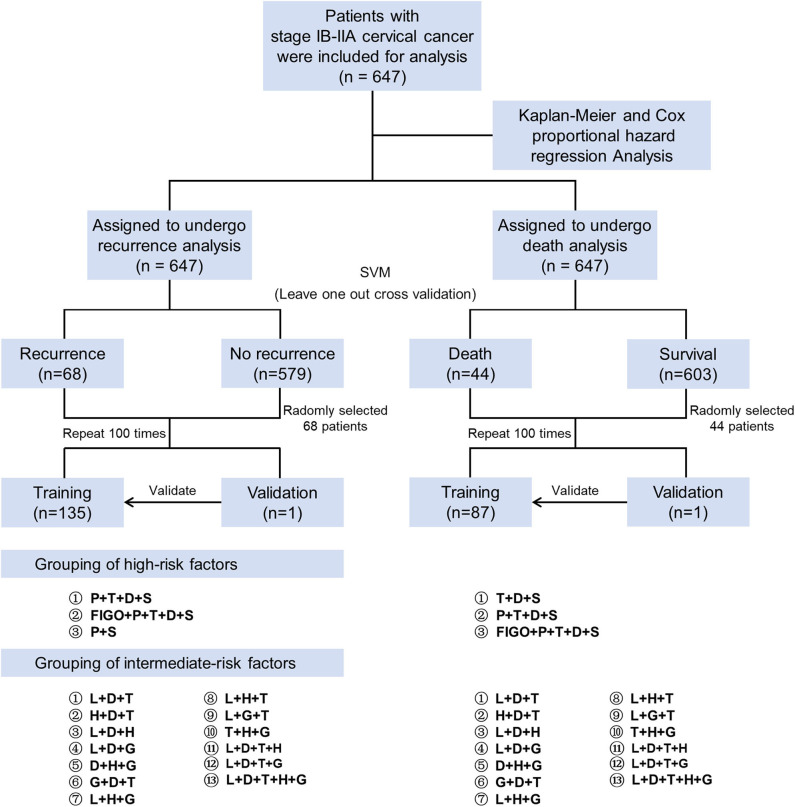
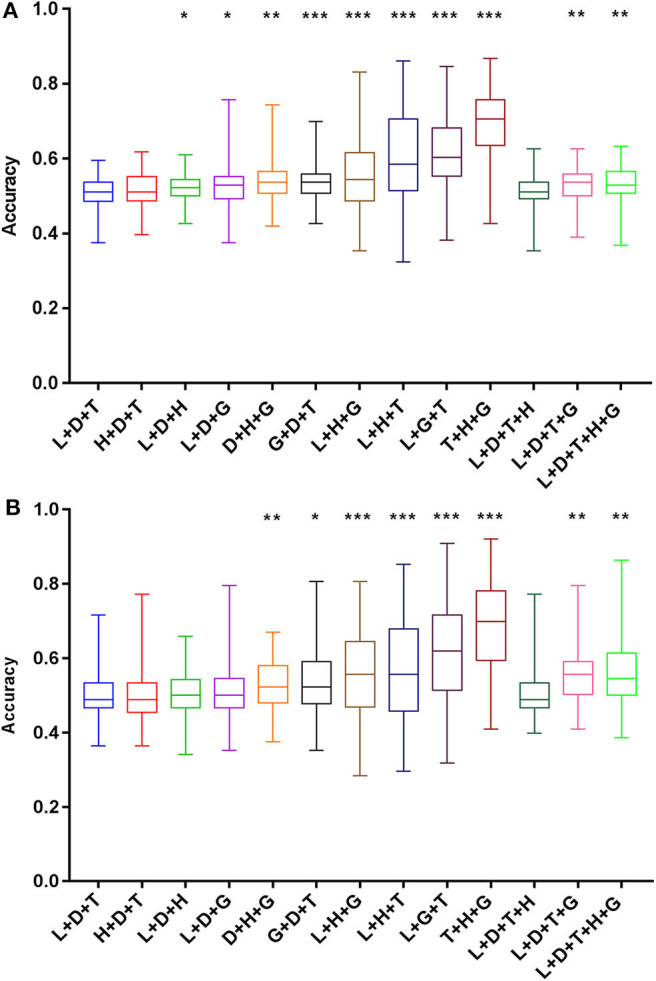
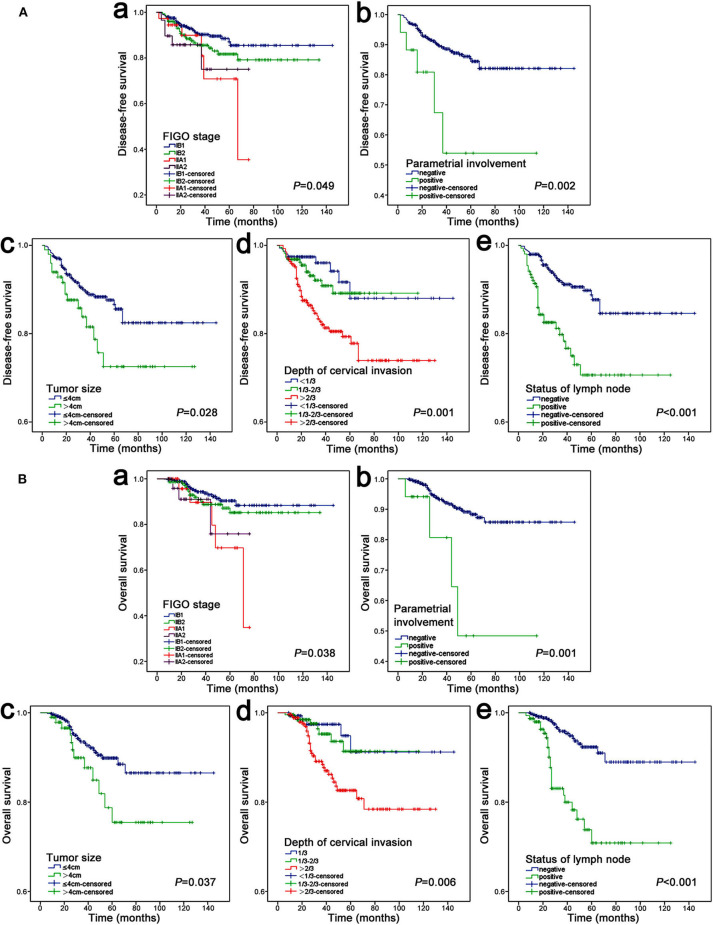
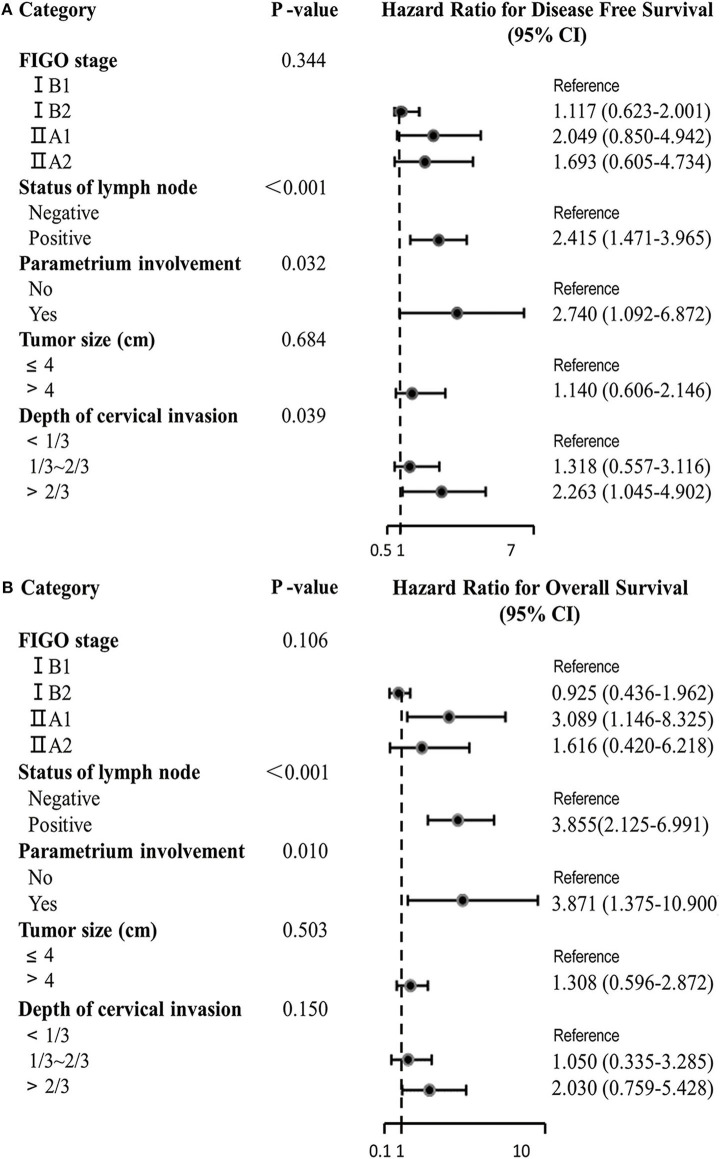
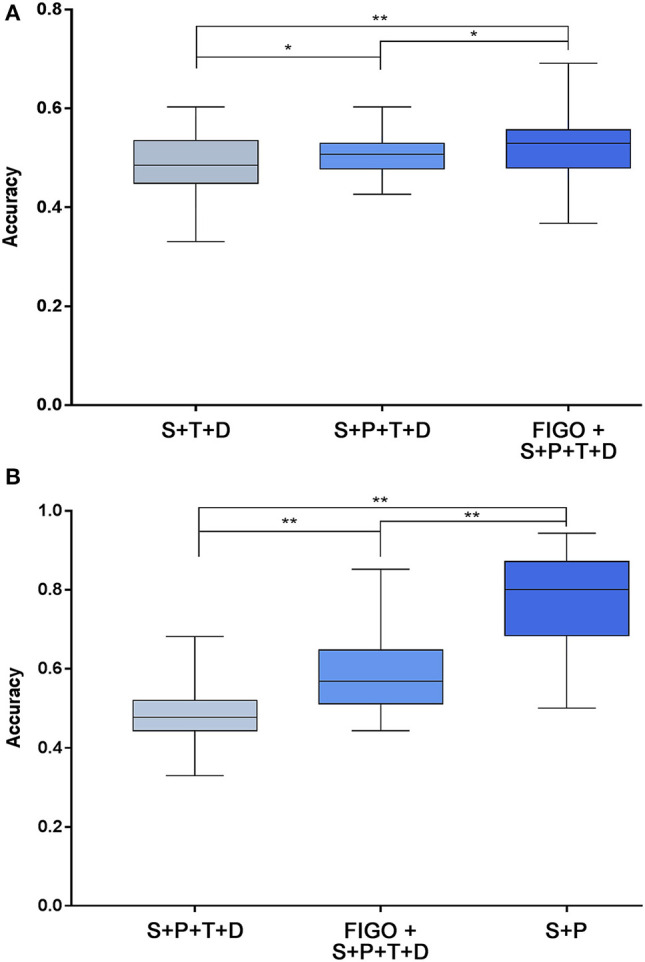
The International Federation of Gynecology and Obstetrics (FIGO) staging system is considered the most powerful prognostic factor in patients with cervical cancer. In addition, other surgical-pathological risk factors have been demonstrated to have significance in predicting the prognosis of patients. Therefore, the purpose of this study was to investigate the effects of the FIGO staging system and surgical-pathological risk factors on the prognosis of cervical cancer patients. A retrospective study was performed on patients diagnosed with cervical cancer at FIGO stage IB1-IIA2. Kaplan-Meier, Cox proportional hazards regression analysis and the support vector machine (SVM) algorithm were used to assess and validate the high-risk factors related to recurrence and death. A total of 647 patients were included. Kaplan-Meier analysis showed that five high-risk factors, including FIGO stage, status of pelvic lymph node, parametrial involvement, tumor size, and depth of cervical cancer, had a significant effect on the prognosis of patients. In multivariate analysis, pelvic lymph node metastasis (hazard ratio [HR] 2.415, 95% confidence interval [CI] 1.471-3.965), parametrial involvement (HR 2.740, 95% CI 1.092-6.872) and >2/3 depth of cervical invasion (HR 2.263, 95% CI 1.045-4.902) were three independent risk factors of disease-free survival. Pelvic lymph node metastasis (HR 3.855, 95% CI 2.125-6.991) and parametrial involvement (HR 3.871, 95% CI 1.375-10.900) were two independent risk factors for overall survival. When all five high-risk factors were assembled and used for classification prediction through SVM, it achieved the highest prediction accuracy of recurrence (accuracy = 69.1%). The highest prediction accuracy for survival was 94.3% when only using the two independent predictors (the pathological status of lymph nodes and parametrium involvement) by SVM classifiers. Among the 13 groups of intermediate-risk factor, the combination of tumor size, histology and grade of differentiation was more accurate in predicting prognosis than the intermediate-risk factors in the Sedlis criteria (recurrence: 86.8% vs. 60.0%; death: 92.0% vs. 71.6%). The combination of FIGO stage and surgical-pathological risk factors can further enhance the prediction accuracy of the prognosis in patients with early-stage cervical cancer. Histology and grade of differentiation can further improve the prediction accuracy of intermediate-risk factors in the Sedlis criteria.
国际妇产科联盟(FIGO)分期系统被认为是宫颈癌患者最有力的预后因素。此外,其他手术病理危险因素已被证明对预测患者预后具有重要意义。因此,本研究的目的是探讨FIGO分期系统和手术病理危险因素对宫颈癌患者预后的影响。对FIGO分期为IB1-IIA2期的宫颈癌患者进行了一项回顾性研究。采用Kaplan-Meier法、Cox比例风险回归分析和支持向量机(SVM)算法评估和验证与复发和死亡相关的高危因素。共纳入647例患者。Kaplan-Meier分析显示,包括FIGO分期、盆腔淋巴结状态、宫旁组织受累情况、肿瘤大小和宫颈癌浸润深度在内的五个高危因素对患者预后有显著影响。多因素分析中,盆腔淋巴结转移(风险比[HR]2.415,95%置信区间[CI]1.471-3.965)、宫旁组织受累(HR 2.740,95%CI 1.092-6.872)和宫颈癌浸润深度>2/3(HR 2.263,95%CI 1.045-4.902)是无病生存的三个独立危险因素。盆腔淋巴结转移(HR 3.855,95%CI 2.125-6.991)和宫旁组织受累(HR 3.871,95%CI 1.375-10.900)是总生存的两个独立危险因素。当将所有五个高危因素组合并通过SVM进行分类预测时,其复发预测准确率最高(准确率=69.1%)。当仅使用两个独立预测因素(淋巴结和宫旁组织的病理状态)通过SVM分类器进行生存预测时,最高预测准确率为94.3%。在13组中危因素中,肿瘤大小、组织学类型和分化程度的组合在预测预后方面比Sedlis标准中的中危因素更准确(复发:86.8%对60.0%;死亡:92.0%对71.6%)。FIGO分期和手术病理危险因素的组合可进一步提高早期宫颈癌患者预后的预测准确率。组织学类型和分化程度可进一步提高Sedlis标准中危因素的预测准确率。