Institute for Health Policy and Organisation, Centre for Primary Care and Health Services Research, School of Health Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester, UK.
Institute for Health Policy and Organisation, School of Health Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester, UK.
JAMA Netw Open. 2020 Aug 3;3(8):e2015009. doi: 10.1001/jamanetworkopen.2020.15009.
An effective and sustainable hearing loss (HL) screening strategy for the early detection of and intervention for HL in older adults is needed.
To examine the concordance of self-reported measures of hearing difficulty with objective hearing data and the factors associated with the potential discordances among these measures across different population subgroups of a representative sample of people 50 years and older in England.
DESIGN, SETTING, AND PARTICIPANTS: This study was a cross-sectional analysis of wave 7 of the English Longitudinal Study of Ageing (ELSA), a large, population-based, prospective cohort study that provides a unique resource for exploring issues associated with aging in England in the 21st century. The full analytic cohort was composed of 9666 individuals participating in the ELSA wave 7, which collected information from June 1, 2014, to May 31, 2015. This study further analyzed a sample of 8529 adults 50 to 89 years of age who had an assessment of their hearing by self-reported measures, and consented to assessment by a qualified nurse via a hearing screening device, and did not have an ear infection or a cochlear implant. Bivariate analyses were performed from July 1 to December 30, 2018, and multivariate analysis from January 1 to June 30, 2019. Multiple logistic regression models examined factors associated with misclassification of hearing difficulties across several categories among those with objectively identified HL.
The study examined whether age, marital status, retirement status, indicators of socioeconomic position, and lifestyle factors (such as body mass index, physical activity, and tobacco and alcohol consumption) were associated with the concordance between self-reported hearing problems and manual audiometry among older adults.
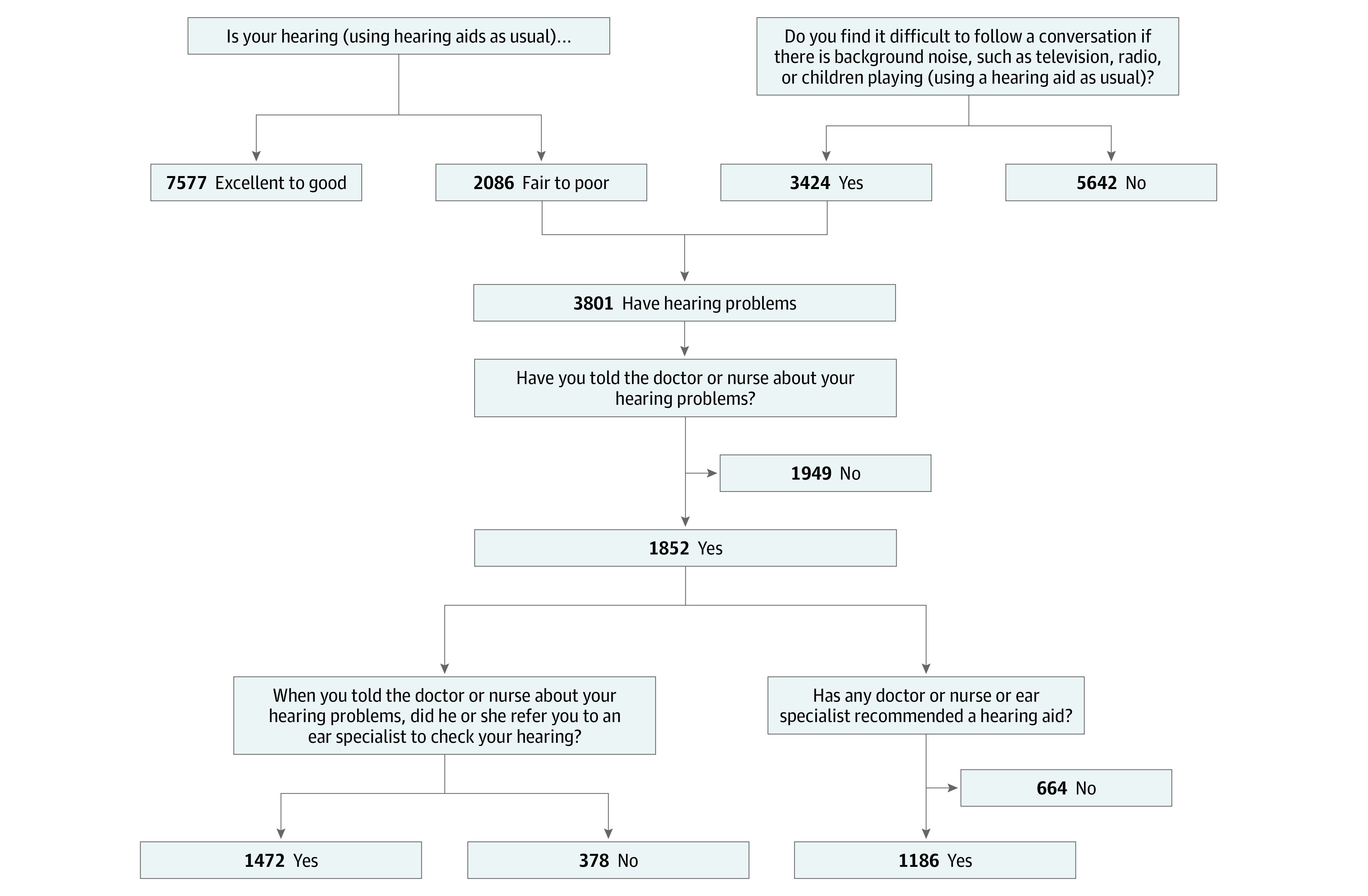
Self-reported hearing measures, including hearing in background noise, compared with objective audiometric assessments.
A total of 9666 study participants (5368 female [55.5%]; mean [SD] age, 67.4 [14.4] years) provided responses regarding their hearing difficulties, hearing in noise, quality of care in hearing, and hearing aid recommendation in ELSA wave 7. Within the cohort, 684 individuals (30.2%) with objectively measured HL greater than 35 dB HL at 3.0 kHz went undetected by the self-report measure, whereas the new constructed categories for moderate and moderately severe or severe HL resulted in 9.3% increased sensitivity. Factors associated with misreporting hearing difficulties (while they had objectively measured HL >35 dB HL at 3.0 kHz, in the better-hearing ear) were as follows: female sex (odds ratio [OR], 1.97; 95% CI, 1.18-3.28), no educational qualifications (OR, 1.37; 95% CI, 1.26-2.55), routine or manual occupation (OR, 1.43; 95% CI, 1.28-2.61), tobacco consumption (OR, 1.14; 95% CI, 1.08-1.90), alcohol intake above the low-risk-level guidelines (OR, 1.13; 95% CI, 1.11-2.34), and lack of moderate physical activity (OR, 1.25; 95% CI, 1.03-1.42). Age was largely associated with misreporting of moderately severe to severe HL; the odds were 5.75 (95% CI, 1.17-8.13) higher for those 65 to 74 years of age and 7.08 (95% CI, 1.41-9.30) higher for those 75 to 89 years of age to not report their hearing difficulties compared with those 50 to 64 years of age. In addition, socioeconomic indicators, such as educational level (OR, 1.95; 95% CI, 1.63-6.01) and occupation (OR, 2.07; 95% CI, 1.78-5.40), along with lifestyle factors, such as smoking (OR, 1.46; 95% CI, 1.25-2.48) and alcohol intake above the low-risk-level guidelines (OR, 1.86; 95% CI, 1.67-5.12), were factors associated with misreporting moderately severe or severe HL.
The use of a screening measure for audiometric testing and a self-report measure is essential for accurately identifying older people with HL. The results of this study should be considered by HL researchers who analyze self-reported hearing data as a surrogate measurement of audiometric hearing to identify bias in their observed analytic research results.
需要一种有效的、可持续的听力损失(HL)筛查策略,以便早期发现老年人的 HL 并进行干预。
本研究旨在调查自我报告的听力困难测量值与客观听力数据的一致性,并探讨在英格兰具有代表性的 50 岁及以上人群的不同亚组中,这些测量值之间潜在差异的相关因素。
设计、地点和参与者:本研究为英国老龄化纵向研究(ELSA)第 7 波的横断面分析,这是一项大型、基于人群的前瞻性队列研究,为探索 21 世纪英国老龄化相关问题提供了独特的资源。全分析队列由参与 ELSA 第 7 波的 9666 名个体组成,该研究于 2014 年 6 月 1 日至 2015 年 5 月 31 日期间收集了信息。本研究进一步分析了 8529 名 50 至 89 岁的成年人样本,他们通过自我报告的措施评估了自己的听力,并同意由合格护士通过听力筛查设备进行评估,且没有耳部感染或人工耳蜗植入。2018 年 7 月 1 日至 12 月 30 日进行了双变量分析,2019 年 1 月 1 日至 6 月 30 日进行了多变量分析。多元逻辑回归模型检验了在客观识别出 HL 的人群中,几个类别中听力困难的分类错误与哪些因素有关。
本研究调查了年龄、婚姻状况、退休状况、社会经济地位指标和生活方式因素(如体重指数、体力活动和烟酒消费)是否与老年人的自我报告听力问题与手动测听之间的一致性有关。
自我报告的听力测量值,包括在背景噪声中的听力,与客观听力评估进行比较。
共有 9666 名研究参与者(5368 名女性[55.5%];平均[SD]年龄 67.4[14.4]岁)在 ELSA 第 7 波中提供了有关听力困难、噪声中听力、听力保健质量和助听器推荐的回答。在队列中,684 名(30.2%)客观测量 HL 大于 3.0 kHz 时的 35 dB HL 的个体未被自我报告的测量方法检出,而新构建的中度和中度至重度或重度 HL 类别导致敏感性提高了 9.3%。与客观测量 HL >3.0 kHz 时(在较好耳朵中)报告听力困难有关的因素包括:女性(比值比[OR],1.97;95%置信区间[CI],1.18-3.28)、无教育资格(OR,1.37;95% CI,1.26-2.55)、常规或手动职业(OR,1.43;95% CI,1.28-2.61)、吸烟(OR,1.14;95% CI,1.08-1.90)、饮酒超过低风险水平指南(OR,1.13;95% CI,1.11-2.34)和缺乏适度体力活动(OR,1.25;95% CI,1.03-1.42)。年龄主要与中度至重度 HL 的报告错误有关;与 50 至 64 岁的个体相比,65 至 74 岁的个体和 75 至 89 岁的个体报告听力困难的可能性分别高 5.75(95% CI,1.17-8.13)和 7.08(95% CI,1.41-9.30)。此外,社会经济指标,如教育水平(OR,1.95;95% CI,1.63-6.01)和职业(OR,2.07;95% CI,1.78-5.40),以及生活方式因素,如吸烟(OR,1.46;95% CI,1.25-2.48)和饮酒超过低风险水平指南(OR,1.86;95% CI,1.67-5.12),是与报告中度或重度 HL 错误相关的因素。
使用听力测试筛查措施和自我报告措施对于准确识别有 HL 的老年人至关重要。本研究的结果应引起分析自我报告听力数据作为听力测量替代指标的 HL 研究人员的注意,以识别其观察性分析研究结果中的偏差。