Zeng Ya, Ni Jianjiao, Yu Fan, Zhou Yue, Zhao Yang, Li Shuyan, Guo Tiantian, Chu Li, Yang Xi, Chu Xiao, Cai Xuwei, Zhu Zhengfei
Department of Radiation Oncology, Fudan University Shanghai Cancer Center, Shanghai, 200032, China.
Department of Radiation Oncology, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, 200030, China.
Radiat Oncol. 2020 Aug 27;15(1):207. doi: 10.1186/s13014-020-01651-y.
There was no study investigating real-world utilization and outcome of LCT in Osimertinib-treated NSCLC with oligo-residual disease. This study was to analyze the clinical value of local consolidative therapy (LCT) in Osimertinib-treated non-small cell lung cancer (NSCLC) patients with oligo-residual disease.
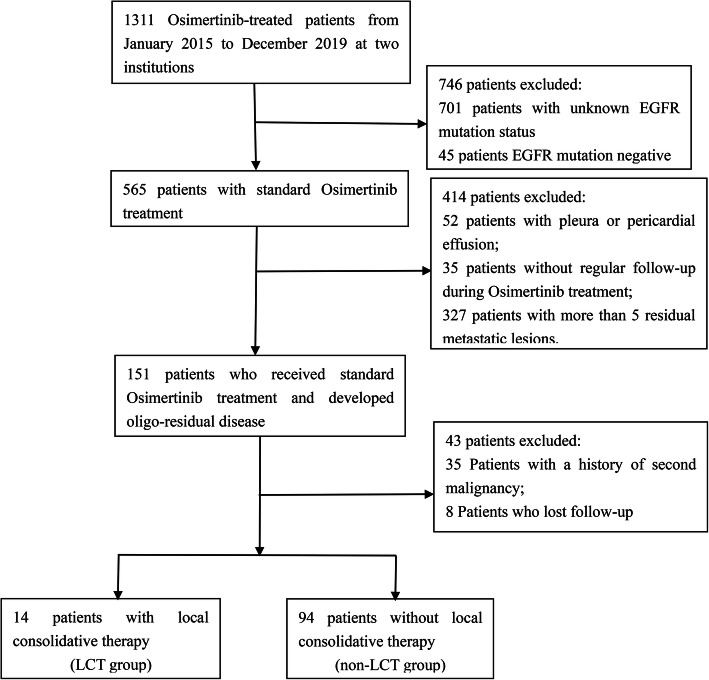
Patients receiving standard Osimertinib treatment and developing oligo-residual disease (five or fewer residual metastatic lesions) were retrospectively reviewed. Local therapies performed to the oligo-residual tumor lesions or primary lung site before Osimertinib treatment failure were considered as LCT.
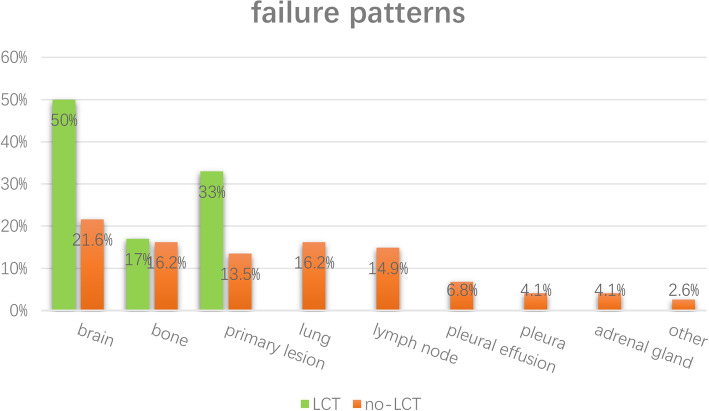
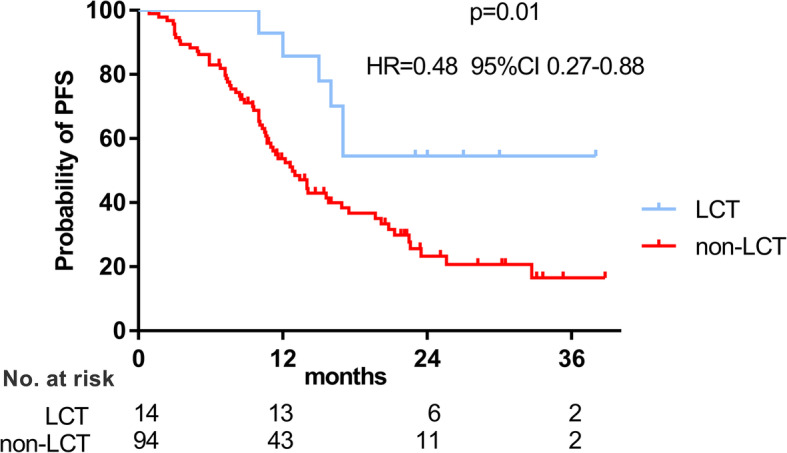
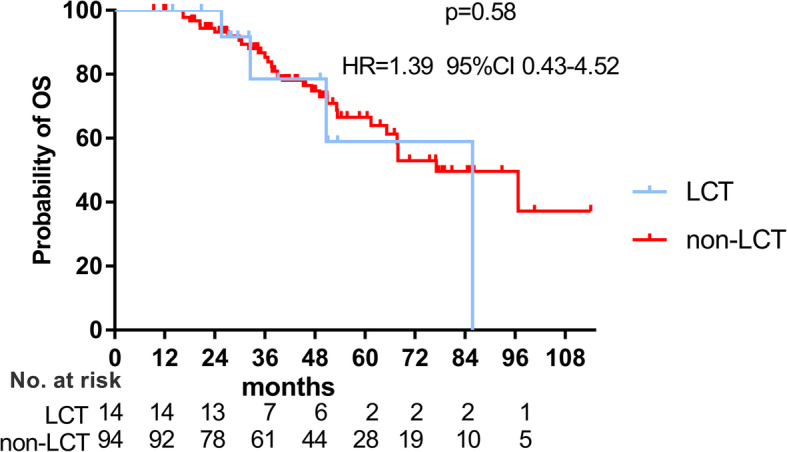
Of 108 patients recruited, first-line and second-line Osimertinib were administered in 25 and 83 patients, respectively, while LCT was performed in 14 patients. With a median follow-up of 43.6 months, 69 patients developed progressive disease. LCT significantly improved progression-free survival (PFS) (NR vs 12.8 months, p = 0.01) and was independently associated with prolonged PFS (HR = 0.29, 95%CI 0.12 to 0.68, p = 0.004). Patients receiving LCT had a numerically longer overall survival (OS) (85.8 vs 77.1 months, p = 0.58) and after adjusting for potentially confounding factors, LCT was associated with a non-significantly prolonged OS (HR = 0.37, 95%CI 0.12-1.16, p = 0.089). Pattern of failure analyses indicated that progressive disease developed at the originally existed oligo-residual lesions in 76.2% of the 63 patients who didn't receive LCT and had Osimertinib treatment failure. Of note, 7 (70%) of the 10 patients who had oligo-residual cranial disease but didn't receive LCT, developed more than five progressive lesions in the brain, which were no longer suitable for stereotactic radiosurgery.
Among Osimertinib-treated NSCLC patients having oligo-residual lesions, LCT could improve local control and significantly increase PFS, which need to be verified by further investigations.
尚无研究调查奥希替尼治疗的寡残留疾病非小细胞肺癌(NSCLC)中局部巩固治疗(LCT)的真实世界应用情况及疗效。本研究旨在分析LCT在奥希替尼治疗的寡残留疾病NSCLC患者中的临床价值。
回顾性分析接受标准奥希替尼治疗并出现寡残留疾病(五个或更少残留转移灶)的患者。在奥希替尼治疗失败前对寡残留肿瘤病灶或原发性肺部位进行的局部治疗被视为LCT。
在纳入的108例患者中,分别有25例和83例接受一线和二线奥希替尼治疗,14例患者接受了LCT。中位随访43.6个月,69例患者出现疾病进展。LCT显著改善了无进展生存期(PFS)(未达到 vs 12.8个月,p = 0.01),且与PFS延长独立相关(风险比[HR]=0.29,95%置信区间[CI] 0.12至0.68,p = 0.004)。接受LCT的患者总生存期(OS)在数值上更长(85.8 vs 77.1个月,p = 0.58),在调整潜在混杂因素后,LCT与OS非显著延长相关(HR = 0.37,95%CI 0.12 - 1.16,p = 0.089)。失败模式分析表明,在63例未接受LCT且奥希替尼治疗失败的患者中,76.2%的患者在原本存在的寡残留病灶处出现疾病进展。值得注意的是,10例有寡残留颅内疾病但未接受LCT的患者中有7例(70%)在脑部出现了超过五个进展性病灶,不再适合立体定向放射外科治疗。
在接受奥希替尼治疗的有寡残留病灶的NSCLC患者中,LCT可改善局部控制并显著提高PFS,这需要进一步研究验证。