Health Policy Research Center, Institute of Health, Shiraz University of Medical Sciences, Shiraz, Iran.
Health Management and Economics Research Center, Iran University of Medical Sciences, Tehran, Iran.
Int J Health Policy Manag. 2022 Apr 1;11(4):443-452. doi: 10.34172/ijhpm.2020.152.
Diabetes imposes an enormous burden on patients, families, societies, and healthcare systems. Determining the affordability of medications is an important complicated and vague task, especially in low- and middle-income countries (LMICs). This study aimed to assess the affordability of diabetes medication therapy in Iran's health system.
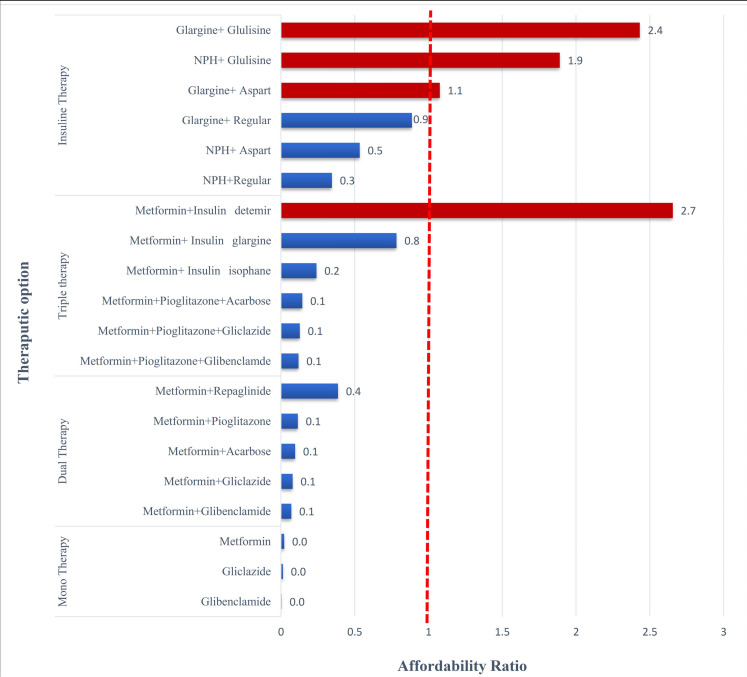
This paper presents a scenario-based assessment of the affordability of all registered anti-diabetes medications in Iran in 2017. To this end, 4 medication therapy scenarios were defined as mono, dual, triple, and insulin therapy in accordance with the existing guidelines and clinicians' opinions. Then the affordability ratio of each treatment scenario was determined for type 1 and type 2 diabetes drawing on the World Health Organization (WHO)/Health Action International (HAI) Methodology. If the affordability ratio for treatment schedules was more than 1, the patients' out-of-pocket (OOP) expenses exceeded the lowest-paid unskilled government worker (LPGW)' wage per day, and the treatment was labelled as non-affordable.
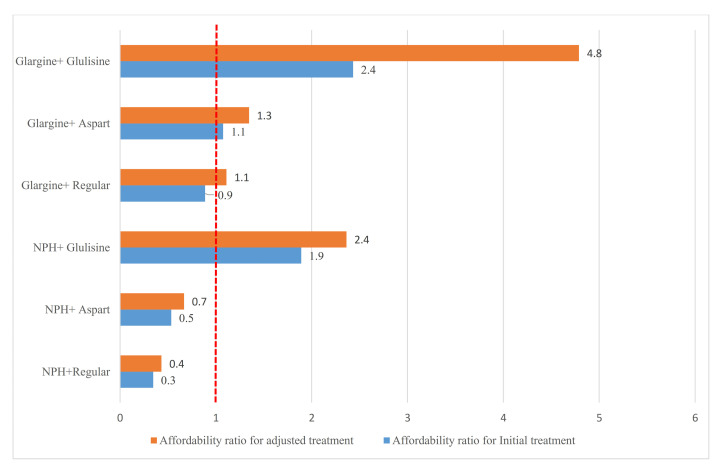
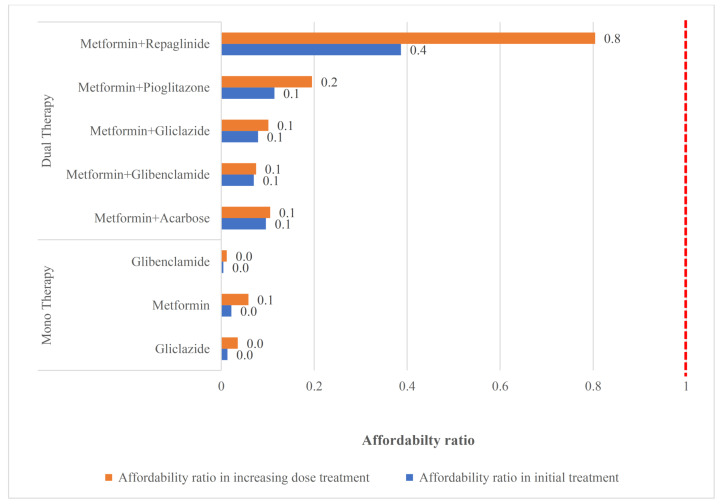
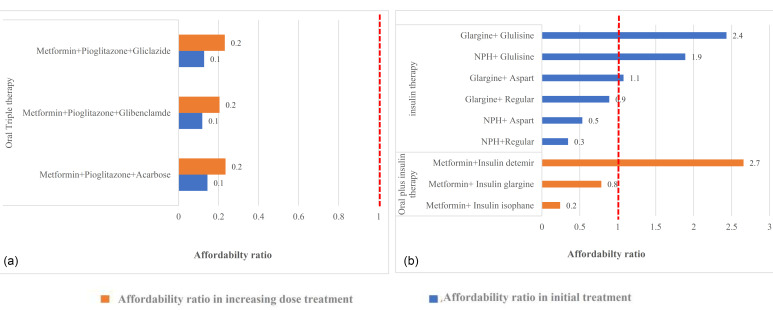
The results revealed that the mono, dual, and triple (non-insulin) medication therapies in type 2 diabetes were affordable, despite an increase in the dosage or a switch from the monotherapy to the combination therapy of oral medications. However, some treatment scenarios in the triple therapy, including oral plus insulin and some insulin only therapies, were proved to be non-affordable. In type 1 diabetes, only insulin glulisine, detemir, and lispro were non-affordable in monotherapy. Regarding the combination therapy, only isophane insulin with aspart or regular insulin were affordable treatments.
Although oral medication therapies were documented to be affordable, insulin therapy, with current coverage conditions, for patients with lowest paid wages and those receiving even less is unaffordable and a major barrier to treatment; hence, policy-maker should consider targeting and more financial protection policies to improve the affordability of insulin therapies among this group of patients.
糖尿病给患者、家庭、社会和医疗保健系统带来了巨大负担。确定药物的可负担性是一项重要而复杂的任务,尤其是在低收入和中等收入国家(LMICs)。本研究旨在评估伊朗卫生系统中糖尿病药物治疗的可负担性。
本研究基于现有的指南和临床医生的意见,根据 4 种药物治疗方案,即单药、二联、三联和胰岛素治疗,对 2017 年伊朗所有注册的抗糖尿病药物的可负担性进行了基于情景的评估。然后,根据世界卫生组织(WHO)/国际健康行动(HAI)方法,确定了 1 型和 2 型糖尿病患者每种治疗方案的可负担性比率。如果治疗方案的可负担性比率超过 1,患者的自付费用超过了最低工资的非熟练工人(LPGW)每天的工资,则该治疗方案被标记为不可负担。
结果表明,2 型糖尿病的单药、二联和三联(非胰岛素)药物治疗是可负担的,尽管剂量增加或从单药治疗改为口服药物联合治疗。然而,一些三联疗法的治疗方案,包括口服药物加胰岛素和一些仅胰岛素的治疗方案,被证明是不可负担的。在 1 型糖尿病中,只有赖脯胰岛素、门冬胰岛素和甘精胰岛素在单药治疗时是不可负担的。对于联合治疗,只有与门冬氨酸或常规胰岛素联合使用的精蛋白锌胰岛素是可负担的治疗方案。
尽管口服药物治疗被证明是可负担的,但对于那些收入最低和收入更低的患者来说,胰岛素治疗在现行的覆盖条件下是不可负担的,也是治疗的主要障碍;因此,政策制定者应考虑针对这一人群制定和实施更多的财政保护政策,以提高胰岛素治疗的可负担性。