Section of Cardiovascular Medicine Department of Internal Medicine Yale University School of Medicine New Haven CT.
Center for Outcomes Research and Evaluation Yale New Haven Health Services Corporation New Haven CT.
J Am Heart Assoc. 2020 Sep 15;9(18):e016038. doi: 10.1161/JAHA.120.016038. Epub 2020 Sep 1.
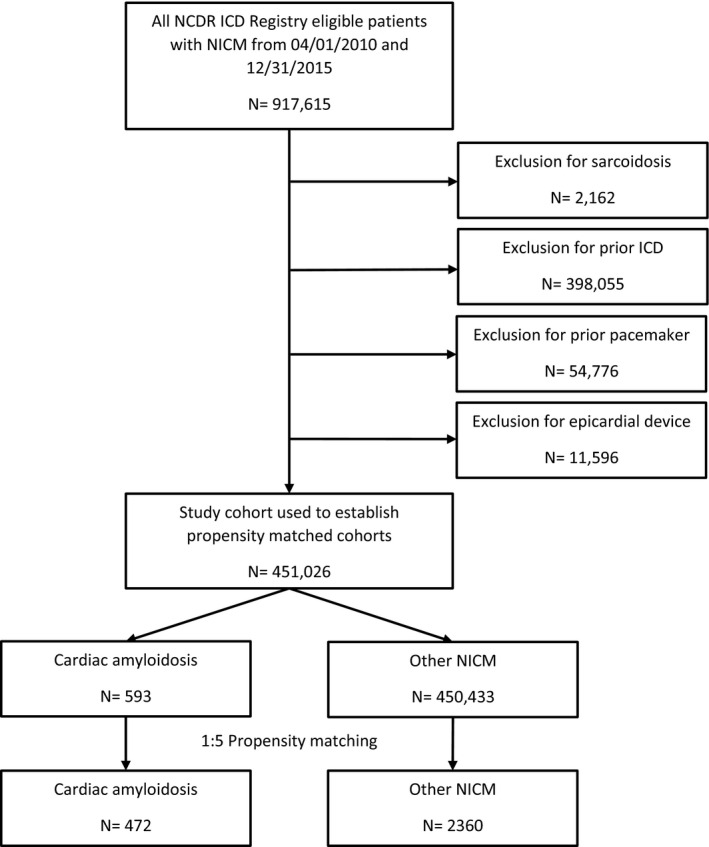
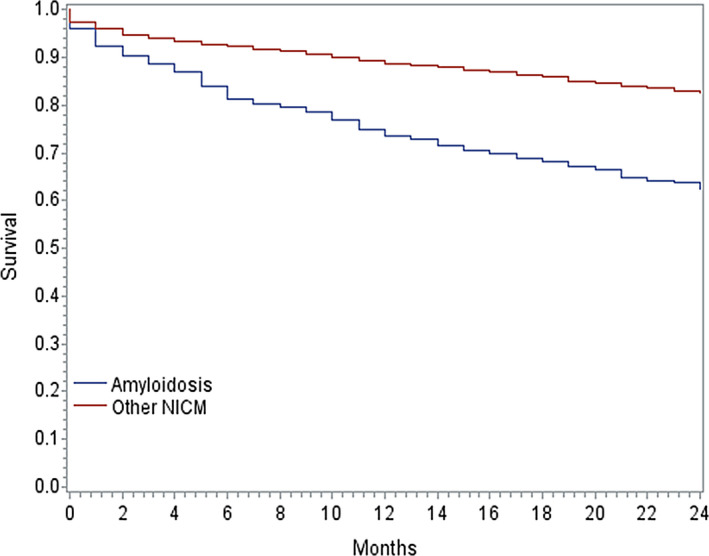
Background Outcomes data in patients with cardiac amyloidosis after implantable cardioverter-defibrillator (ICD) implantation are limited. We compared outcomes of patients with ICDs implanted for cardiac amyloidosis versus nonischemic cardiomyopathies (NICMs) and evaluated factors associated with mortality among patients with cardiac amyloidosis. Methods and Results Using National Cardiovascular Data Registry's ICD Registry data between April 1, 2010 and December 31, 2015, we created a 1:5 propensity-matched cohort of patients implanted with ICDs with cardiac amyloidosis and NICM. We compared mortality between those with cardiac amyloidosis and matched patients with NICM using Kaplan-Meier survival curves and Cox proportional hazards models. We also evaluated risk factors associated with 1-year mortality in patients with cardiac amyloidosis using multivariable Cox proportional hazards regression models. Among 472 patients with cardiac amyloidosis and 2360 patients with propensity-matched NICMs, 1-year mortality was significantly higher in patients with cardiac amyloidosis compared with patients with NICMs (26.9% versus 11.3%, <0.001). After adjustment for covariates, cardiac amyloidosis was associated with a significantly higher risk of all-cause mortality (hazard ratio [HR], 1.80; 95% CI, 1.56-2.08). In a multivariable analysis of patients with cardiac amyloidosis, several factors were significantly associated with mortality: syncope (HR, 1.78; 95% CI, 1.22-2.59), ventricular tachycardia (HR, 1.65; 95% CI, 1.15-2.38), cerebrovascular disease (HR, 2.03; 95% CI, 1.28-3.23), diabetes mellitus (HR, 1.55; 95% CI, 1.05-2.27), creatinine = 1.6 to 2.5 g/dL (HR, 1.99; 95% CI, 1.32-3.02), and creatinine >2.5 (HR, 4.34; 95% CI, 2.72-6.93). Conclusions Mortality after ICD implantation is significantly higher in patients with cardiac amyloidosis than in patients with propensity-matched NICMs. Factors associated with death among patients with cardiac amyloidosis include prior syncope, ventricular tachycardia, cerebrovascular disease, diabetes mellitus, and impaired renal function.
植入式心脏复律除颤器(ICD)植入后心脏淀粉样变患者的预后数据有限。我们比较了心脏淀粉样变患者与非缺血性心肌病(NICM)患者的 ICD 植入结局,并评估了心脏淀粉样变患者死亡的相关因素。
利用国家心血管数据登记 ICD 登记数据(2010 年 4 月 1 日至 2015 年 12 月 31 日),我们创建了一个 1:5 比例的心脏淀粉样变和 NICM 患者 ICD 植入倾向性匹配队列。我们使用 Kaplan-Meier 生存曲线和 Cox 比例风险模型比较了心脏淀粉样变患者与 NICM 匹配患者的死亡率。我们还使用多变量 Cox 比例风险回归模型评估了心脏淀粉样变患者 1 年死亡率的相关因素。在 472 例心脏淀粉样变患者和 2360 例匹配的 NICM 患者中,心脏淀粉样变患者的 1 年死亡率明显高于 NICM 患者(26.9%比 11.3%,<0.001)。在调整了协变量后,心脏淀粉样变与全因死亡率显著升高相关(风险比[HR],1.80;95%CI,1.56-2.08)。在心脏淀粉样变患者的多变量分析中,几个因素与死亡率显著相关:晕厥(HR,1.78;95%CI,1.22-2.59)、室性心动过速(HR,1.65;95%CI,1.15-2.38)、脑血管疾病(HR,2.03;95%CI,1.28-3.23)、糖尿病(HR,1.55;95%CI,1.05-2.27)、肌酐 1.6-2.5 g/dL(HR,1.99;95%CI,1.32-3.02)和肌酐 >2.5 g/dL(HR,4.34;95%CI,2.72-6.93)。
与匹配的 NICM 患者相比,心脏淀粉样变患者 ICD 植入后的死亡率显著更高。心脏淀粉样变患者死亡的相关因素包括既往晕厥、室性心动过速、脑血管疾病、糖尿病和肾功能不全。