Department of Urology, Zhujiang Hospital, Southern Medical University, Guangzhou, China.
Cancer Med. 2020 Oct;9(20):7590-7600. doi: 10.1002/cam4.3404. Epub 2020 Sep 1.
Bladder cancer (BCa) is the most common urinary malignancy. The standard surgical treatment for patients with muscle-invasive BCa is cystectomy plus urinary diversion. Ileal conduit (IC) or orthotopic neobladder (ON), which have different indications, are the most commonly performed urinary diversions.
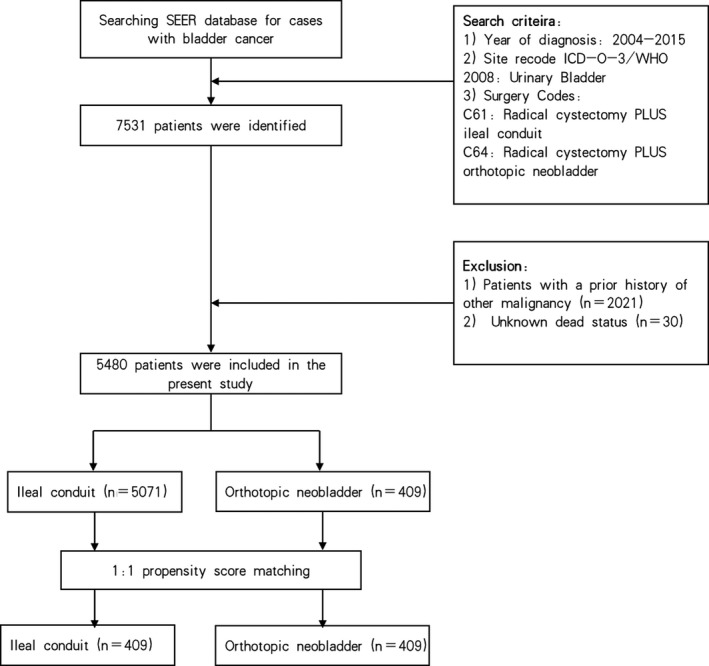
We sampled 5480 BCa patients from the Surveillance, Epidemiology, and End Results (SEER) database from 2004 to 2015. Kaplan-Meier method with the log-rank test was used to assess cancer-specific survival (CSS) and overall survival (OS). Univariate and multivariate Cox's proportional hazard model was conducted to evaluate the hazard ratio of cancer-specific mortality and all-cause mortality before and after propensity score matching (PSM).
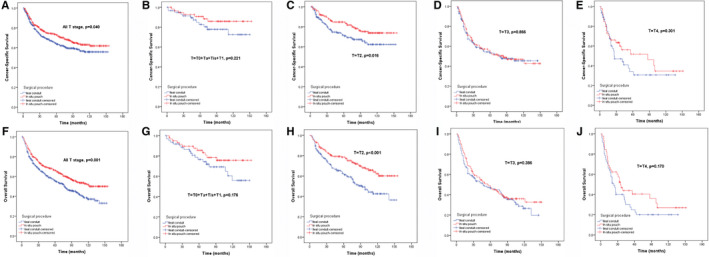
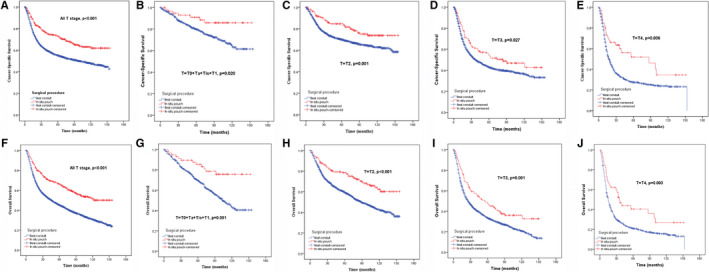
We identified 5480 patients who received radical cystectomy (RC) plus IC (n = 5071) or ON (n = 409) with a median follow-up period of 33 months (interquartile range, 13-78 months). Patients in the ON group tended to be male and younger, with a higher percentage of married individuals, early pathological T stage, lymphadenectomy, and non-radiotherapy (all P < .05). After 1:1 PSM, 409 matched pairs were selected. Univariate and multivariate analysis showed that the ON group had better CSS and OS probabilities than the IC group in the overall cohort [hazard ratio (HR): 0.692, 95% confidence intervals (CI): 0.576-0.831, P < .001; HR: 0.677, 95% CI: 0.579-0.793, P < .001 respectively]. However, subgroup analysis revealed that only patients with pathological T2 stage benefited from ON diversion after PSM in the context of CSS (P = .016) and OS (P <.001).
Young, married, and male patients with early pathological T stage, especially T2 stage, were more suitable to receive RC plus ON surgery, which could improve their probability of survival.
膀胱癌(BCa)是最常见的泌尿系统恶性肿瘤。肌层浸润性膀胱癌患者的标准手术治疗是膀胱切除术加尿流改道。回肠导管(IC)或原位新膀胱(ON)是最常用的尿流改道术,它们有不同的适应证。
我们从 2004 年至 2015 年的监测、流行病学和最终结果(SEER)数据库中抽取了 5480 例 BCa 患者。采用 Kaplan-Meier 法和对数秩检验评估癌症特异性生存(CSS)和总生存(OS)。采用单因素和多因素 Cox 比例风险模型评估倾向评分匹配(PSM)前后癌症特异性死亡率和全因死亡率的风险比。
我们共确定了 5480 例接受根治性膀胱切除术(RC)加 IC(n=5071)或 ON(n=409)的患者,中位随访时间为 33 个月(四分位距 13-78 个月)。ON 组患者倾向于男性和年轻,已婚比例较高,病理 T 分期较早,有淋巴结清扫术和未接受放疗(均 P<.05)。1:1 PSM 后,选择了 409 对匹配对。单因素和多因素分析显示,在整个队列中,ON 组的 CSS 和 OS 概率均优于 IC 组[风险比(HR):0.692,95%置信区间(CI):0.576-0.831,P<.001;HR:0.677,95%CI:0.579-0.793,P<.001]。然而,亚组分析显示,仅在 CSS(P=.016)和 OS(P<.001)方面,PSM 后病理 T2 期的患者从 ON 引流中获益。
年轻、已婚和男性、病理 T 分期较早、尤其是 T2 期的患者更适合接受 RC 加 ON 手术,这可以提高他们的生存概率。