Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital and Harvard Medical School, Harvard University, Boston, Massachusetts.
Divisao de Pneumologia, Instituto do Coração, Hospital das Clinícas, Faculdade de Medicina, Universidade de São Paulo, São Paulo, São Paulo, Brazil; and.
Am J Respir Crit Care Med. 2021 Mar 1;203(5):575-584. doi: 10.1164/rccm.201909-1687OC.
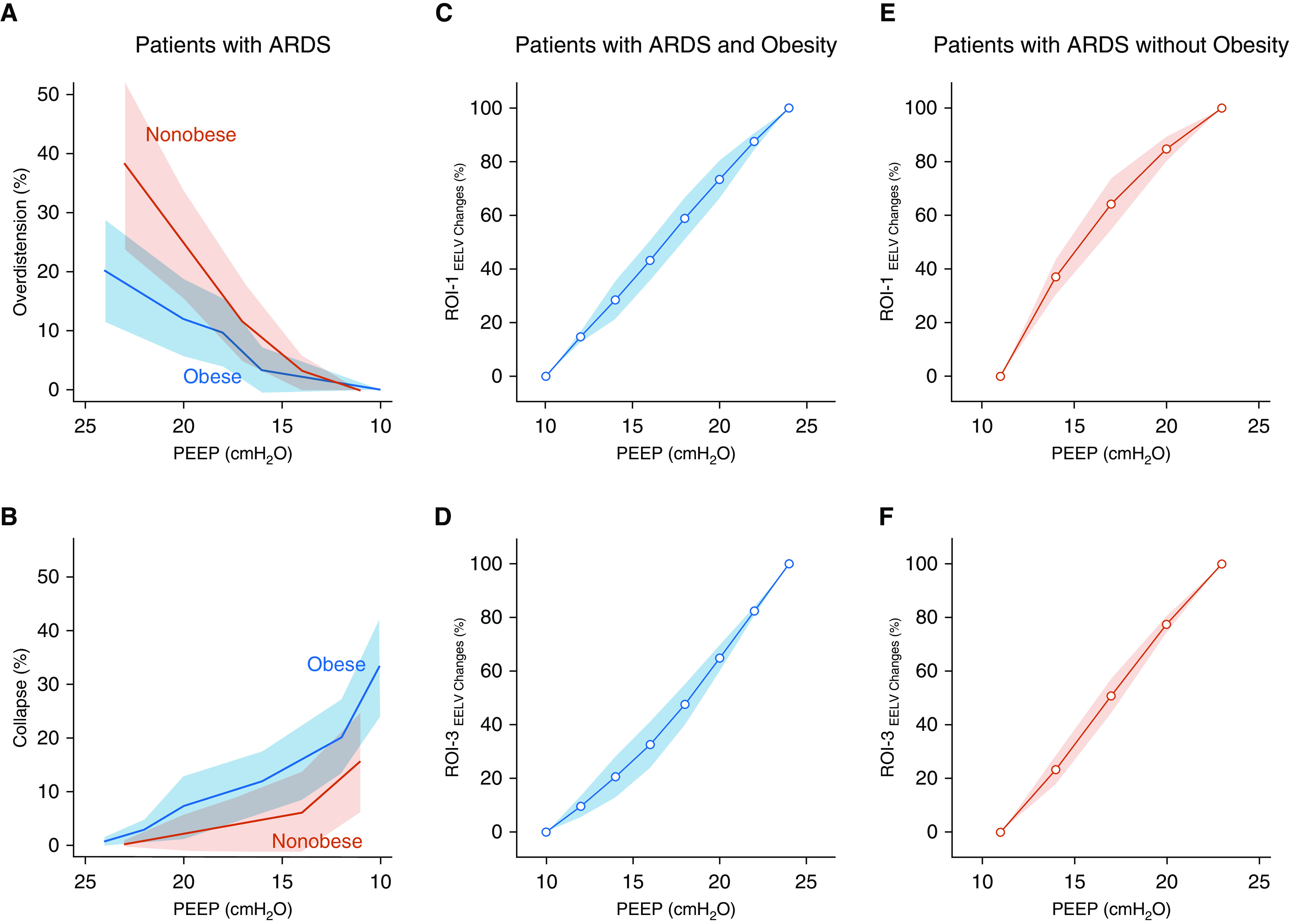
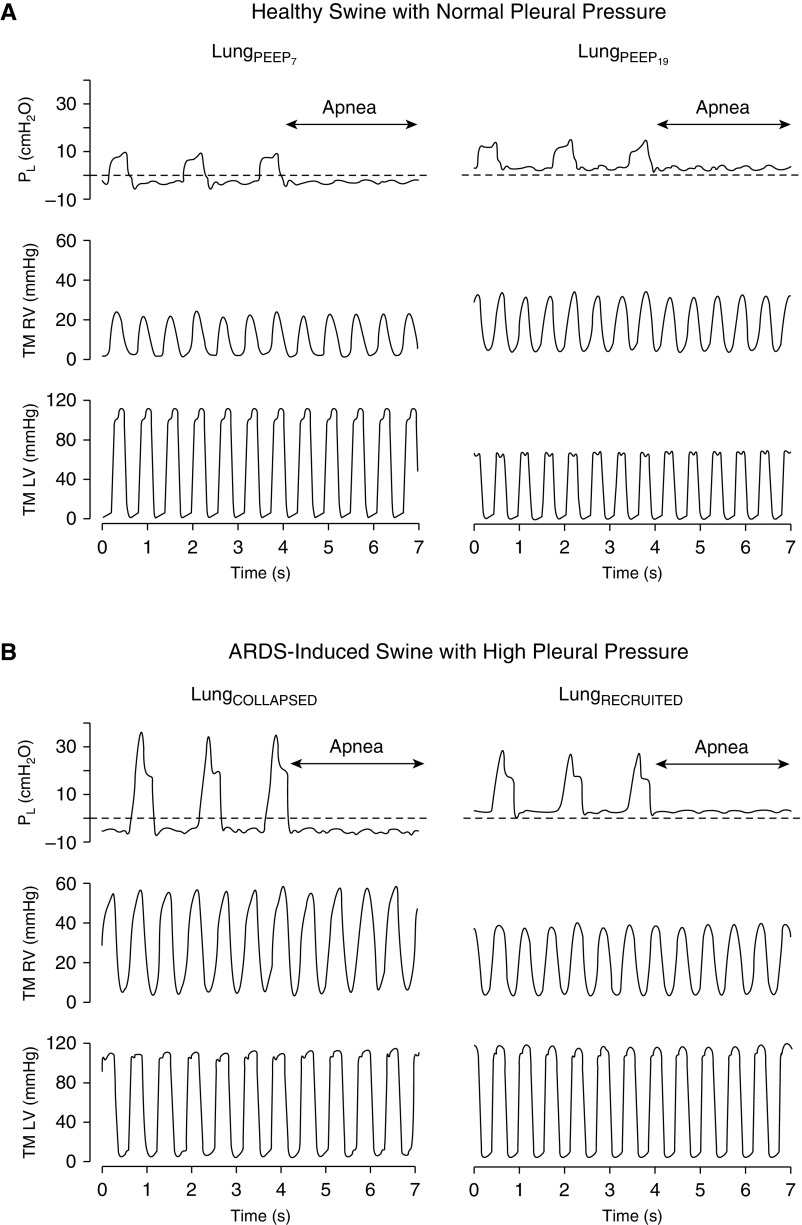
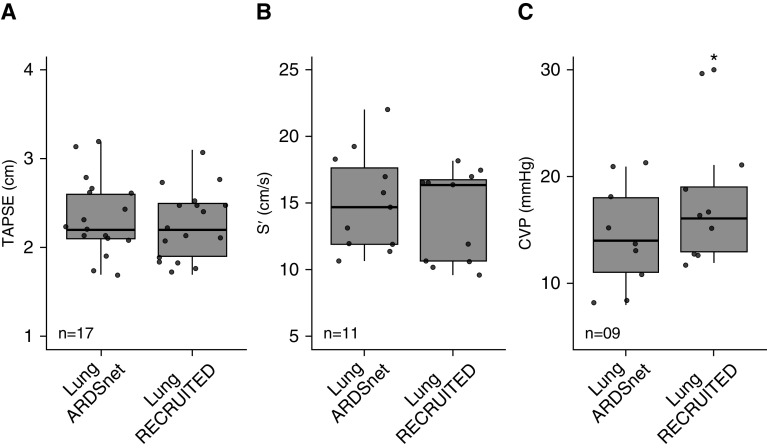
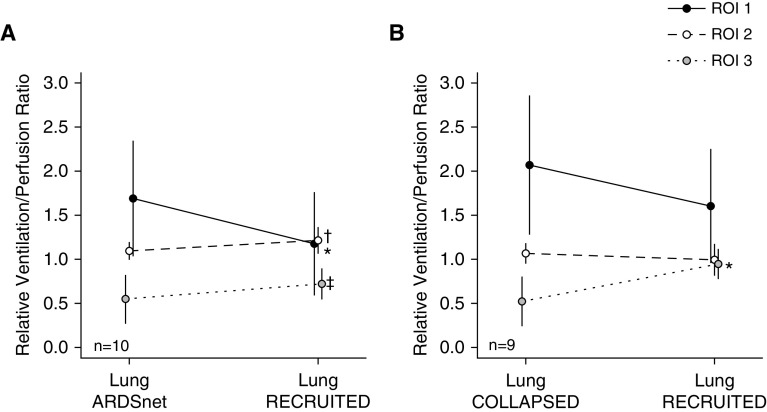
Obesity is characterized by elevated pleural pressure (Ppl) and worsening atelectasis during mechanical ventilation in patients with acute respiratory distress syndrome (ARDS). To determine the effects of a lung recruitment maneuver (LRM) in the presence of elevated Ppl on hemodynamics, left and right ventricular pressure, and pulmonary vascular resistance. We hypothesized that elevated Ppl protects the cardiovascular system against high airway pressure and prevents lung overdistension. First, an interventional crossover trial in adult subjects with ARDS and a body mass index ≥ 35 kg/m ( = 21) was performed to explore the hemodynamic consequences of the LRM. Second, cardiovascular function was studied during low and high positive end-expiratory pressure (PEEP) in a model of swine with ARDS and high Ppl ( = 9) versus healthy swine with normal Ppl ( = 6). Subjects with ARDS and obesity (body mass index = 57 ± 12 kg/m) after LRM required an increase in PEEP of 8 (95% confidence interval [95% CI], 7-10) cm HO above traditional ARDS Network settings to improve lung function, oxygenation and [Formula: see text]/[Formula: see text] matching, without impairment of hemodynamics or right heart function. ARDS swine with high Ppl demonstrated unchanged transmural left ventricular pressure and systemic blood pressure after the LRM protocol. Pulmonary arterial hypertension decreased (8 [95% CI, 13-4] mm Hg), as did vascular resistance (1.5 [95% CI, 2.2-0.9] Wood units) and transmural right ventricular pressure (10 [95% CI, 15-6] mm Hg) during exhalation. LRM and PEEP decreased pulmonary vascular resistance and normalized the [Formula: see text]/[Formula: see text] ratio. High airway pressure is required to recruit lung atelectasis in patients with ARDS and class III obesity but causes minimal overdistension. In addition, patients with ARDS and class III obesity hemodynamically tolerate LRM with high airway pressure.Clinical trial registered with www.clinicaltrials.gov (NCT02503241).
肥胖症的特点是在急性呼吸窘迫综合征(ARDS)患者机械通气期间,胸内压升高和肺不张加重。为了确定在胸内压升高的情况下,肺复张手法(LRM)对血流动力学、左心室和右心室压力以及肺血管阻力的影响。我们假设,升高的胸内压可保护心血管系统免受高气道压力的影响,并防止过度充气。首先,对肥胖症(BMI≥35kg/m)的成人 ARDS 患者进行了一项介入性交叉试验,以探索 LRM 的血流动力学后果。其次,在 ARDS 模型中研究了低和高呼气末正压(PEEP)期间的心血管功能,该模型中 ARDS 患者的胸内压升高(=9)与正常胸内压的健康猪(=6)进行了比较。LRM 后肥胖症(BMI=57±12kg/m)的 ARDS 患者需要将 PEEP 增加 8(95%置信区间[95%CI],7-10)cm H2O,高于传统 ARDS 网络设置,以改善肺功能、氧合和 PaO2/FiO2 匹配,而不影响血流动力学或右心功能。高胸内压的 ARDS 猪在 LRM 方案后,左心室壁压力和全身血压保持不变。肺动脉高压下降(8[95%CI,13-4]mmHg),血管阻力(1.5[95%CI,2.2-0.9]Wood 单位)和右心室壁压力(10[95%CI,15-6]mmHg)也下降。呼气时 LRM 和 PEEP 降低了肺血管阻力并使 PaO2/FiO2 比值正常化。需要高气道压力来复张 ARDS 伴 III 级肥胖患者的肺不张,但仅引起最小的过度充气。此外,肥胖症(BMI≥35kg/m)的 ARDS 患者在高气道压力下也能耐受 LRM。该临床试验在 www.clinicaltrials.gov(NCT02503241)上注册。