Fietz Daniela, Pilatz Adrian, Diemer Thorsten, Wagenlehner Florian, Bergmann Martin, Schuppe Hans-Christian
Institute for Veterinary Anatomy, Histology and Embryology, Justus Liebig University Giessen, Frankfurter Straße 98, 35392 Giessen, Germany.
Hessian Centre of Reproductive Medicine, Justus Liebig University Giessen, 35392 Giessen, Germany.
Basic Clin Androl. 2020 Sep 1;30:13. doi: 10.1186/s12610-020-00111-7. eCollection 2020.
Clomiphene citrate has been proposed as pre-treatment for infertile men with non-obstructive, testicular azoospermia (NOA) before surgery for testicular sperm extraction (TESE), especially when serum testosterone is low.
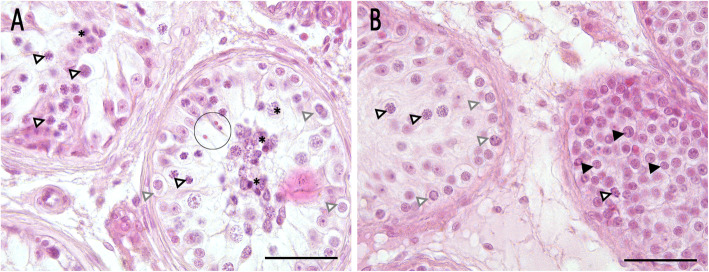
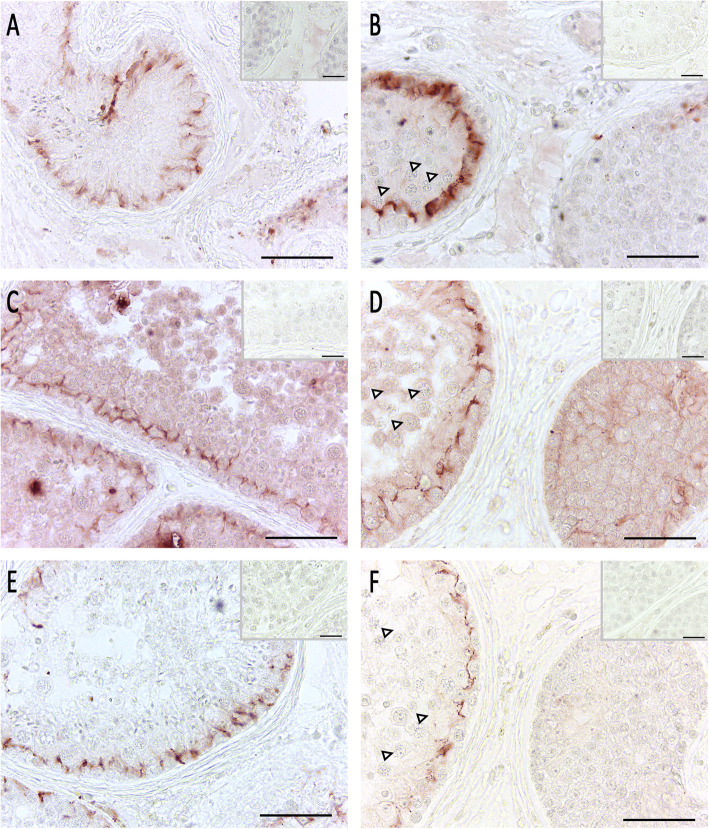
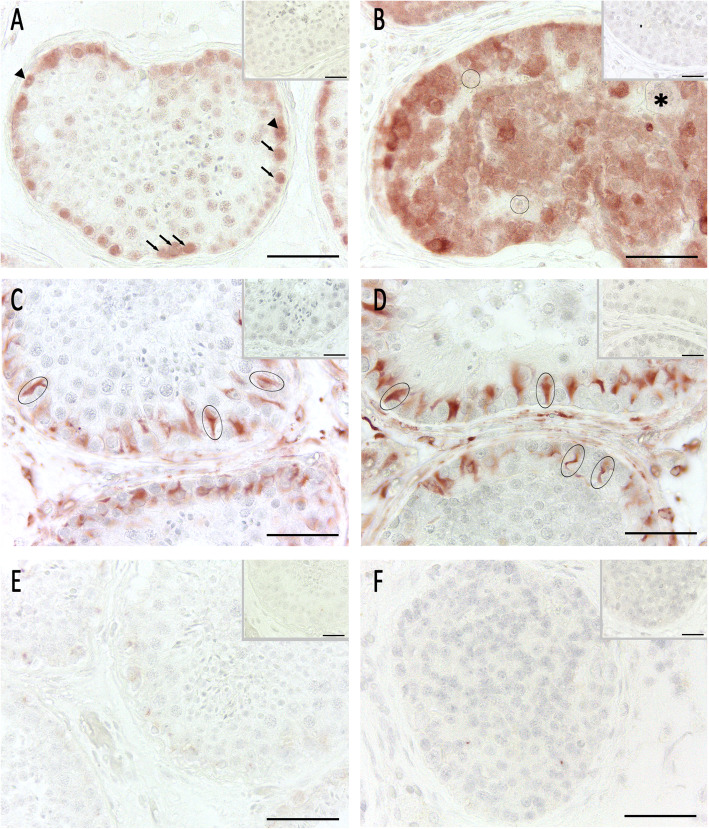
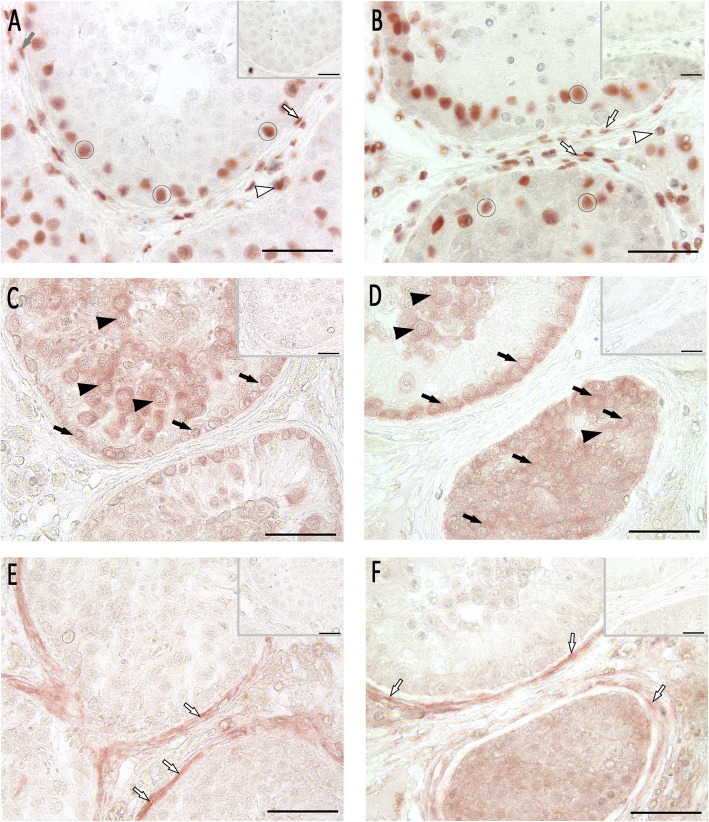
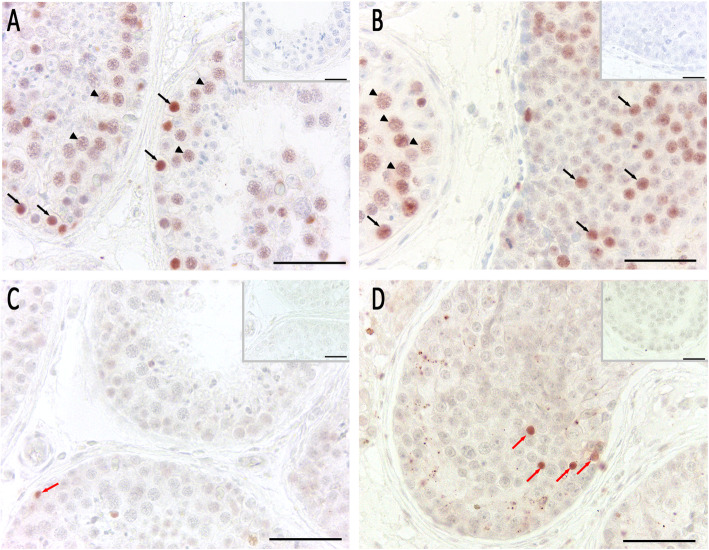
Here, we report on a 33-year old azoospermic patient with a previous history of repeated "fresh" TESE and clomiphene citrate therapy (50 mg/day over 6 months) before undergoing microscopically assisted, bilateral testicular biopsy. Comprehensive histological and immunohistochemical work-up revealed a heterogeneous spermatogenic arrest at the level of spermatogonia or primary spermatocytes, with focally preserved spermatogenesis up to elongated spermatids in the right testis. In the left testis, the majority of tubules (> 70%) showed no tubular lumen or regular seminiferous epithelium but a great number of spermatogonia-like cells. These cells proved to be normally differentiated spermatogonia (positive for melanoma associated antigen 4 (MAGEA4), negative for placental alkaline phosphatase (PlAP)) with increased proliferative activity (positive for proliferating cell nuclear antigen (PCNA)) and a slightly higher rate of apoptotic cells. When compared to a tissue control with normal spermatogenesis, expression of sex hormone receptors androgen receptor (AR), estrogen receptor (ER) alpha, and G-protein coupled estrogen receptor 1 (GPER1) was not altered in patient samples. Sertoli cells appeared to be mature (positive for vimentin, negative for cytokeratin 18), whereas the expression of zona occludens protein 1 (ZO-1), claudin 11, and connexin 43 was absent or dislocated in the tubules with abundance of spermatogonia.
This result suggests that formation of the blood-testis barrier is disturbed in affected tubules. To our knowledge this is the first observation of excessive, non-malignant proliferation of spermatogonia in a NOA patient. Although underlying molecular mechanisms remain to be elucidated, we hypothesize that the unusual pathology was triggered by the high-dose clomiphene citrate treatment preceding testicular biopsy.
枸橼酸氯米芬已被提议作为非梗阻性睾丸无精子症(NOA)不育男性在进行睾丸精子提取术(TESE)手术前的预处理方法,尤其是当血清睾酮水平较低时。
在此,我们报告一名33岁的无精子症患者,该患者此前有多次“新鲜”TESE病史,并在接受显微镜辅助双侧睾丸活检前接受了枸橼酸氯米芬治疗(50毫克/天,持续6个月)。全面的组织学和免疫组化检查显示,生精阻滞异质性地发生在精原细胞或初级精母细胞水平,右侧睾丸局部保留了直至长形精子细胞的生精过程。在左侧睾丸中,大多数曲细精管(>70%)没有管腔或规则的生精上皮,但有大量精原细胞样细胞。这些细胞被证明是正常分化的精原细胞(黑色素瘤相关抗原4(MAGEA4)阳性,胎盘碱性磷酸酶(PlAP)阴性),增殖活性增加(增殖细胞核抗原(PCNA)阳性),凋亡细胞率略高。与具有正常生精功能的组织对照相比,患者样本中性激素受体雄激素受体(AR)、雌激素受体(ER)α和G蛋白偶联雌激素受体1(GPER1)的表达没有改变。支持细胞似乎成熟(波形蛋白阳性,细胞角蛋白18阴性), 而在含有大量精原细胞的曲细精管中,闭合蛋白1(ZO-1)、紧密连接蛋白11和连接蛋白43的表达缺失或错位。
该结果表明,受影响的曲细精管中血睾屏障的形成受到干扰。据我们所知,这是首次在一名NOA患者中观察到精原细胞过度的非恶性增殖。尽管潜在的分子机制仍有待阐明,但我们推测这种异常病理是由睾丸活检前的高剂量枸橼酸氯米芬治疗引发的。