Department of Radiology, University of Washington, Seattle.
Department of Neurological Surgery, University of Washington, Seattle.
JAMA Netw Open. 2020 Sep 1;3(9):e2015713. doi: 10.1001/jamanetworkopen.2020.15713.
Lumbar spine imaging frequently reveals findings that may seem alarming but are likely unrelated to pain. Prior work has suggested that inserting data on the prevalence of imaging findings among asymptomatic individuals into spine imaging reports may reduce unnecessary subsequent interventions.
To evaluate the impact of including benchmark prevalence data in routine spinal imaging reports on subsequent spine-related health care utilization and opioid prescriptions.
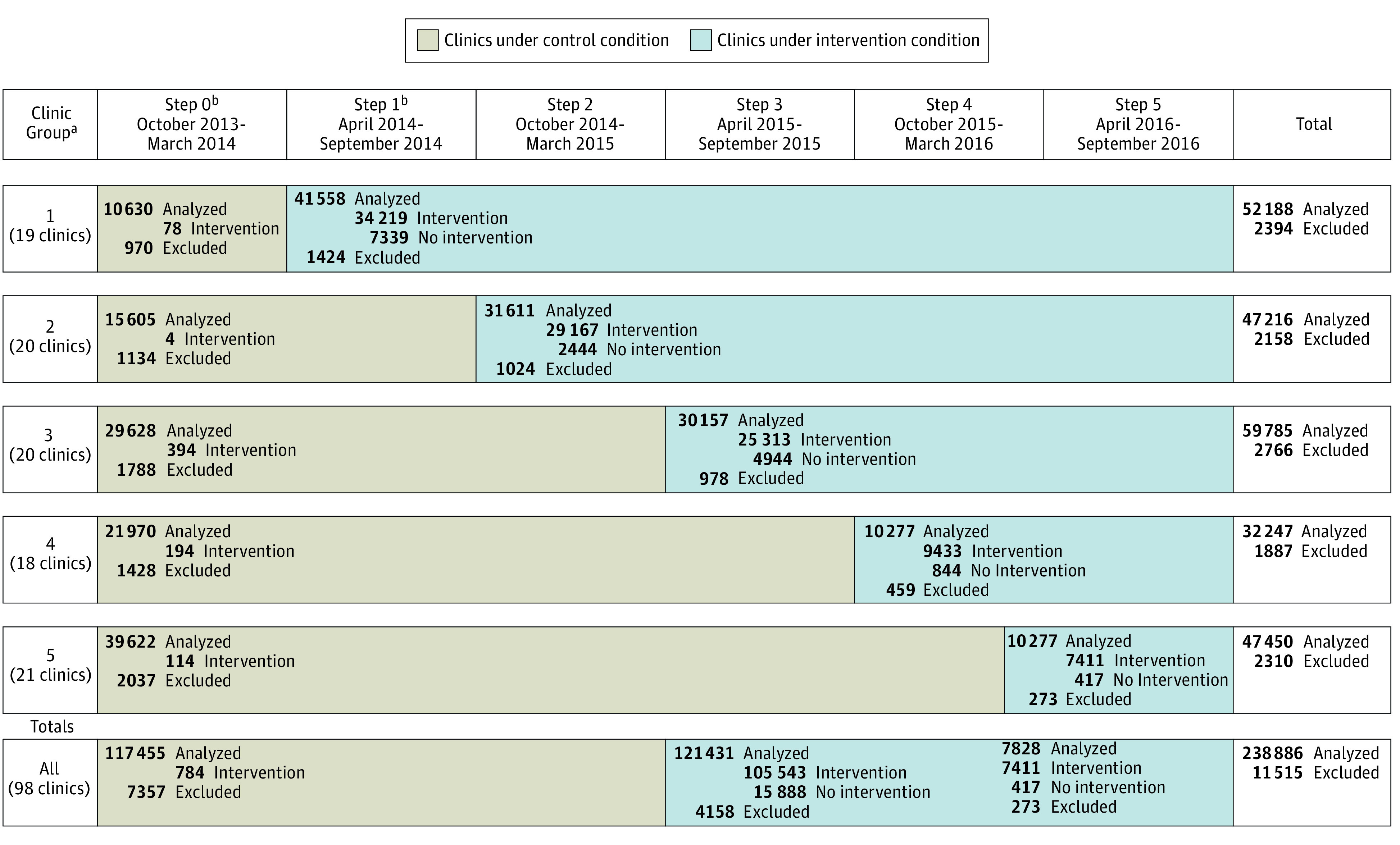
DESIGN, SETTING, AND PARTICIPANTS: This stepped-wedge, pragmatic randomized clinical trial included 250 401 adult participants receiving care from 98 primary care clinics at 4 large health systems in the United States. Participants had imaging of their backs between October 2013 and September 2016 without having had spine imaging in the prior year. Data analysis was conducted from November 2018 to October 2019.
Either standard lumbar spine imaging reports (control group) or reports containing age-appropriate prevalence data for common imaging findings in individuals without back pain (intervention group).
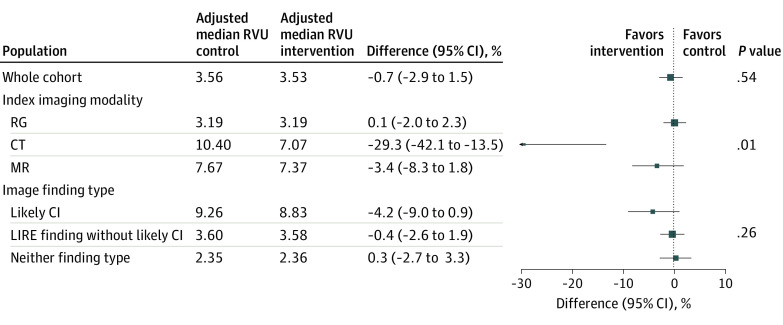
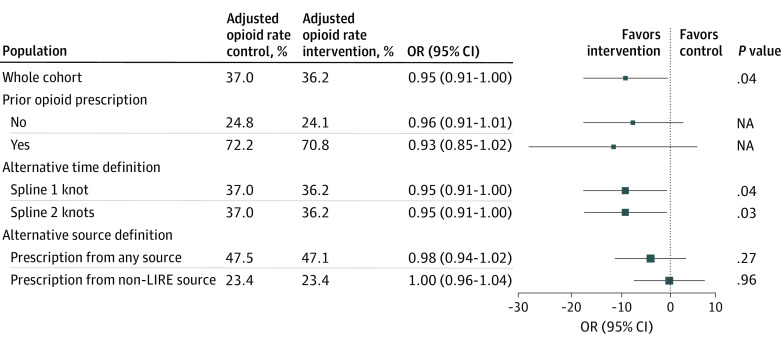
Health care utilization was measured in spine-related relative value units (RVUs) within 365 days of index imaging. The number of subsequent opioid prescriptions written by a primary care clinician was a secondary outcome, and prespecified subgroup analyses examined results by imaging modality.
We enrolled 250 401 participants (of whom 238 886 [95.4%] met eligibility for this analysis, with 137 373 [57.5%] women and 105 497 [44.2%] aged >60 years) from 3278 primary care clinicians. A total of 117 455 patients (49.2%) were randomized to the control group, and 121 431 patients (50.8%) were randomized to the intervention group. There was no significant difference in cumulative spine-related RVUs comparing intervention and control conditions through 365 days. The adjusted median (interquartile range) RVU for the control group was 3.56 (2.71-5.12) compared with 3.53 (2.68-5.08) for the intervention group (difference, -0.7%; 95% CI, -2.9% to 1.5%; P = .54). Rates of subsequent RVUs did not differ between groups by specific clinical findings in the report but did differ by type of index imaging (eg, computed tomography: difference, -29.3%; 95% CI, -42.1% to -13.5%; magnetic resonance imaging: difference, -3.4%; 95% CI, -8.3% to 1.8%). We observed a small but significant decrease in the likelihood of opioid prescribing from a study clinician within 1 year of the intervention (odds ratio, 0.95; 95% CI, 0.91 to 1.00; P = .04).
In this study, inserting benchmark prevalence information in lumbar spine imaging reports did not decrease subsequent spine-related RVUs but did reduce subsequent opioid prescriptions. The intervention text is simple, inexpensive, and easily implemented.
ClinicalTrials.gov Identifier: NCT02015455.
腰椎影像学检查经常会发现一些可能令人担忧但与疼痛无关的结果。先前的研究表明,将无症状个体影像学表现的流行率数据纳入脊柱影像学报告中,可能会减少不必要的后续干预。
评估在常规脊柱影像学报告中纳入基准流行率数据对后续脊柱相关医疗保健利用和阿片类药物处方的影响。
设计、设置和参与者:这是一项阶梯式、实用的随机临床试验,纳入了美国 4 家大型医疗系统的 98 家初级保健诊所的 250401 名成年参与者。这些参与者在 2013 年 10 月至 2016 年 9 月期间接受了背部影像学检查,但在此前一年没有进行过脊柱影像学检查。数据分析于 2018 年 11 月至 2019 年 10 月进行。
标准腰椎影像学报告(对照组)或包含无背痛个体常见影像学表现的年龄适宜流行率数据的报告(干预组)。
在索引影像学检查后 365 天内,以脊柱相关相对价值单位(RVUs)衡量医疗保健利用情况。初级保健临床医生随后开具的阿片类药物处方数量是次要结局,预设定的亚组分析按影像学方式检查结果。
我们从 3278 名初级保健临床医生纳入了 250401 名参与者(其中 238863 名符合本分析条件,137373 名女性,105497 名年龄>60 岁)。共有 117455 名患者(49.2%)被随机分配至对照组,121431 名患者(50.8%)被随机分配至干预组。通过 365 天,干预和对照条件下脊柱相关 RVUs 的累积量没有显著差异。对照组的中位(四分位距)RVU 为 3.56(2.71-5.12),而干预组为 3.53(2.68-5.08)(差值,-0.7%;95%CI,-2.9%至 1.5%;P=0.54)。报告中的具体临床发现并没有导致两组之间后续 RVUs 率的差异,但与索引影像学类型有关(例如,计算机断层扫描:差值,-29.3%;95%CI,-42.1%至-13.5%;磁共振成像:差值,-3.4%;95%CI,-8.3%至 1.8%)。我们观察到研究临床医生在干预后 1 年内开具阿片类药物处方的可能性略有但显著降低(比值比,0.95;95%CI,0.91 至 1.00;P=0.04)。
在这项研究中,在腰椎影像学报告中插入基准流行率信息并没有减少后续脊柱相关 RVUs,但确实减少了后续阿片类药物处方。干预文本简单、廉价,易于实施。
ClinicalTrials.gov 标识符:NCT02015455。