Department of Surgery, Erasmus MC University Medical Center, 's Gravendijkwal 230, 3015 CE, Rotterdam, The Netherlands.
Laboratory for Experimental Oncology and Radiobiology, Amsterdam UMC, University of Amsterdam and Cancer Center Amsterdam, Meibergdreef 9, 1105AZ, Amsterdam, The Netherlands.
BMC Cancer. 2020 Sep 4;20(1):850. doi: 10.1186/s12885-020-07316-z.
There are profound individual differences in clinical outcomes between colorectal cancers (CRCs) presenting with identical stage of disease. Molecular stratification, in conjunction with the traditional TNM staging, is a promising way to predict patient outcomes. We investigated the interconnectivity between tumor stage and tumor biology reflected by the Consensus Molecular Subtypes (CMSs) in CRC, and explored the possible value of these insights in patients with stage II colon cancer.
We performed a retrospective analysis using clinical records and gene expression profiling in a meta-cohort of 1040 CRC patients. The interconnectivity of tumor biology and disease stage was assessed by investigating the association between CMSs and TNM classification. In order to validate the clinical applicability of our findings we employed a meta-cohort of 197 stage II colon cancers.
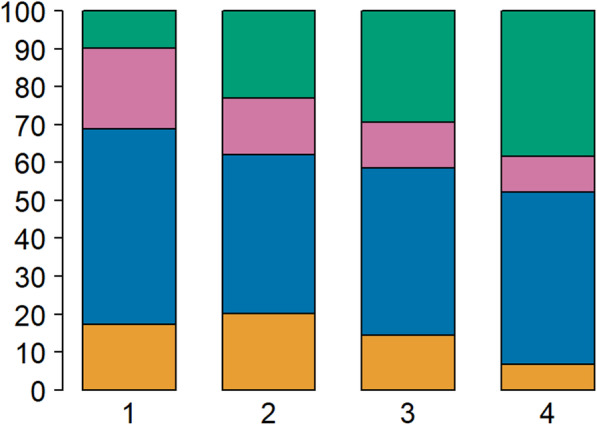
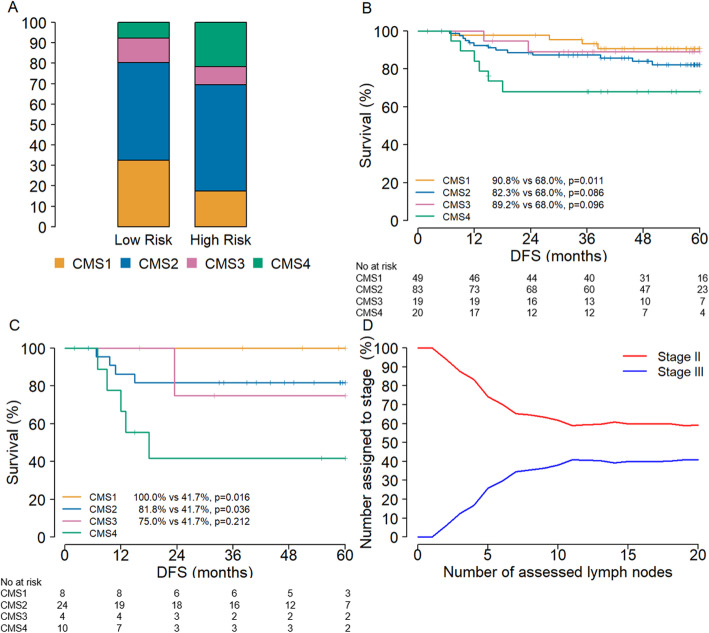
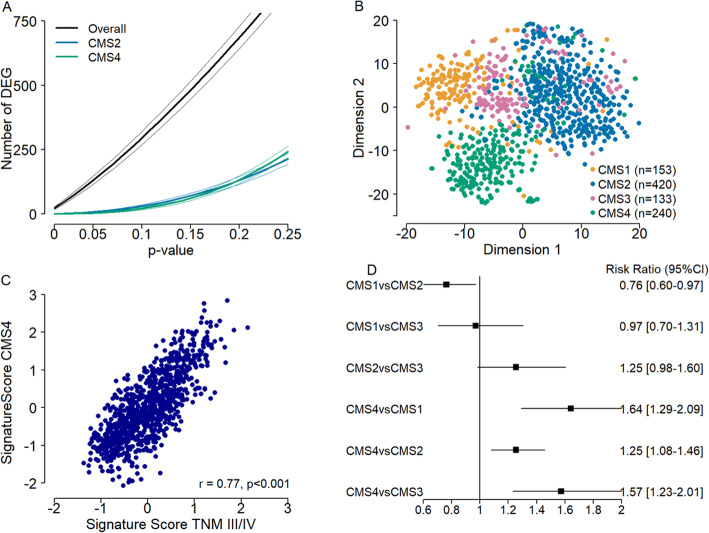
CMS4 was significantly more prevalent in advanced stages of disease (stage I 9.8% versus stage IV 38.5%, p < 0.001). The observed differential gene expression between cancer stages is at least partly explained by the biological differences as reflected by CMS subtypes. Gene signatures for stage III-IV and CMS4 were highly correlated (r = 0.77, p < 0.001). CMS4 cancers showed an increased progression rate to more advanced stages (CMS4 compared to CMS2: 1.25, 95% CI: 1.08-1.46). Patients with a CMS4 cancer had worse survival in the high-risk stage II tumors compared to the total stage II cohort (5-year DFS 41.7% versus 100.0%, p = 0.008).
Considerable interconnectivity between tumor biology and tumor stage in CRC exists. This implies that the TNM stage, in addition to the stage of progression, might also reflect distinct biological disease entities. These insights can potentially be utilized to optimize identification of high-risk stage II colon cancers.
在表现出相同疾病阶段的结直肠癌(CRC)患者中,临床结果存在显著的个体差异。分子分层与传统的 TNM 分期相结合,是预测患者预后的一种很有前途的方法。我们研究了 CRC 中肿瘤分期与肿瘤生物学之间的相互关系,这些肿瘤生物学由共识分子亚型(CMS)反映,并探讨了这些见解在 II 期结肠癌患者中的可能价值。
我们对 1040 例 CRC 患者的临床记录和基因表达谱进行了回顾性分析。通过研究 CMS 与 TNM 分类之间的关联,评估肿瘤生物学与疾病分期之间的相互关系。为了验证我们研究结果的临床适用性,我们还对 197 例 II 期结肠癌患者进行了荟萃分析。
CMS4 在疾病的晚期阶段更为普遍(I 期 9.8%,IV 期 38.5%,p<0.001)。观察到的癌症分期之间的差异表达至少部分由 CMS 亚型反映的生物学差异解释。III-IV 期和 CMS4 的基因特征高度相关(r=0.77,p<0.001)。CMS4 癌症向更晚期进展的速度增加(CMS4 与 CMS2 相比:1.25,95%CI:1.08-1.46)。与总 II 期队列相比,CMS4 癌症患者在高危 II 期肿瘤中的生存较差(5 年 DFS:41.7%与 100.0%,p=0.008)。
CRC 中肿瘤生物学与肿瘤分期之间存在相当大的相互关系。这意味着 TNM 分期除了进展阶段外,还可能反映出不同的生物学疾病实体。这些见解可能有助于优化高危 II 期结肠癌的识别。