Dienstmann R, Mason M J, Sinicrope F A, Phipps A I, Tejpar S, Nesbakken A, Danielsen S A, Sveen A, Buchanan D D, Clendenning M, Rosty C, Bot B, Alberts S R, Milburn Jessup J, Lothe R A, Delorenzi M, Newcomb P A, Sargent D, Guinney J
Computational Oncology, Sage Bionetworks, Seattle, USA.
Oncology Data Science Group, Vall d´Hebron Institute of Oncology and Vall d'Hebron University Hospital, Universitat Autònoma de Barcelona, Barcelona, Spain.
Ann Oncol. 2017 May 1;28(5):1023-1031. doi: 10.1093/annonc/mdx052.
TNM staging alone does not accurately predict outcome in colon cancer (CC) patients who may be eligible for adjuvant chemotherapy. It is unknown to what extent the molecular markers microsatellite instability (MSI) and mutations in BRAF or KRAS improve prognostic estimation in multivariable models that include detailed clinicopathological annotation.
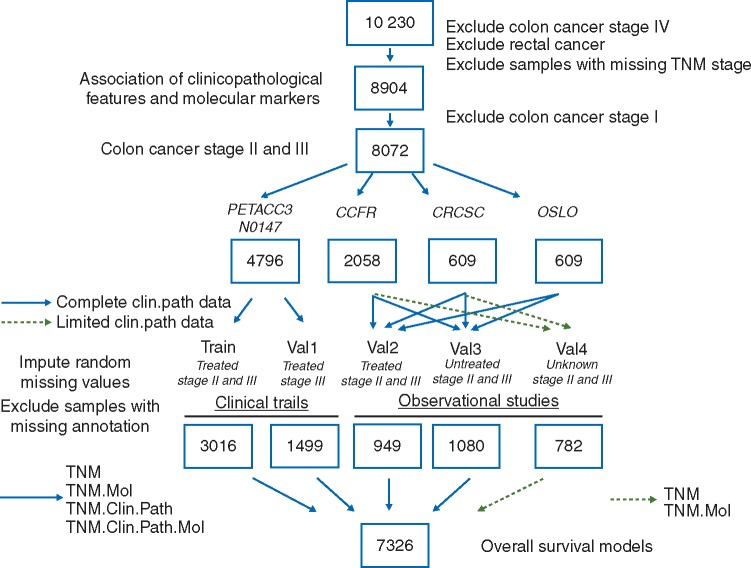
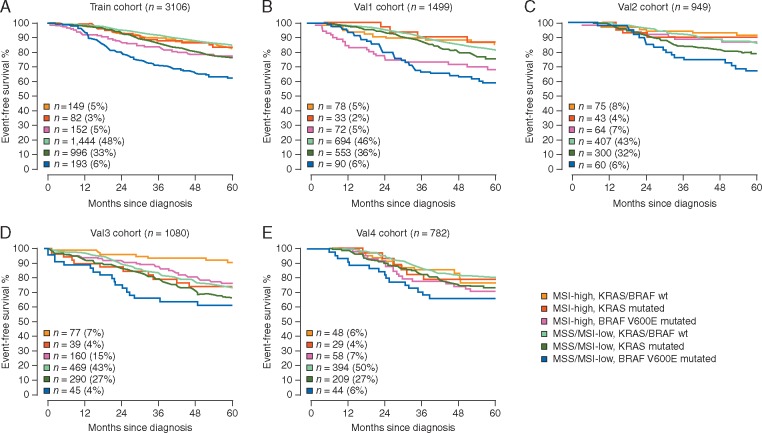
After imputation of missing at random data, a subset of patients accrued in phase 3 trials with adjuvant chemotherapy (n = 3016)-N0147 (NCT00079274) and PETACC3 (NCT00026273)-was aggregated to construct multivariable Cox models for 5-year overall survival that were subsequently validated internally in the remaining clinical trial samples (n = 1499), and also externally in different population cohorts of chemotherapy-treated (n = 949) or -untreated (n = 1080) CC patients, and an additional series without treatment annotation (n = 782).
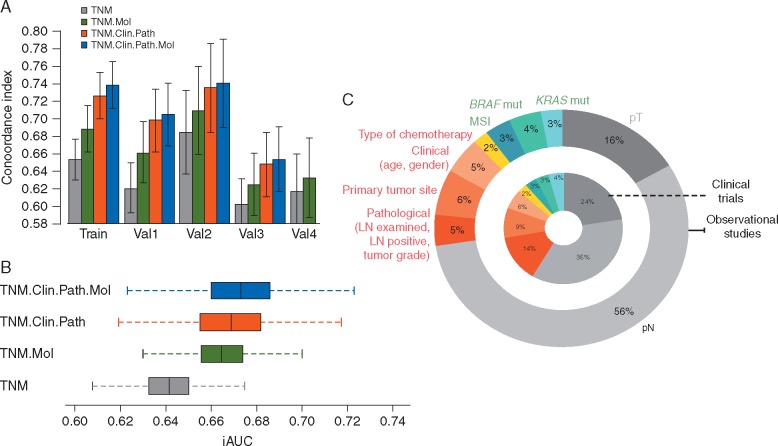
TNM staging, MSI and BRAFV600E mutation status remained independent prognostic factors in multivariable models across clinical trials cohorts and observational studies. Concordance indices increased from 0.61-0.68 in the TNM alone model to 0.63-0.71 in models with added molecular markers, 0.65-0.73 with clinicopathological features and 0.66-0.74 with all covariates. In validation cohorts with complete annotation, the integrated time-dependent AUC rose from 0.64 for the TNM alone model to 0.67 for models that included clinicopathological features, with or without molecular markers. In patient cohorts that received adjuvant chemotherapy, the relative proportion of variance explained (R2) by TNM, clinicopathological features and molecular markers was on an average 65%, 25% and 10%, respectively.
Incorporation of MSI, BRAFV600E and KRAS mutation status to overall survival models with TNM staging improves the ability to precisely prognosticate in stage II and III CC patients, but only modestly increases prediction accuracy in multivariable models that include clinicopathological features, particularly in chemotherapy-treated patients.
单独的TNM分期并不能准确预测可能适合辅助化疗的结肠癌(CC)患者的预后。目前尚不清楚分子标志物微卫星不稳定性(MSI)以及BRAF或KRAS突变在包含详细临床病理注释的多变量模型中能在多大程度上改善预后估计。
在对随机缺失的数据进行插补后,将3期辅助化疗试验(n = 3016)——N0147(NCT00079274)和PETACC3(NCT00026273)——中入组的一部分患者汇总,构建5年总生存的多变量Cox模型,随后在其余临床试验样本(n = 1499)中进行内部验证,并在接受化疗(n = 949)或未接受化疗(n = 1080)的CC患者的不同人群队列以及另外一组无治疗注释(n = 782)的患者中进行外部验证。
在各临床试验队列和观察性研究的多变量模型中,TNM分期、MSI和BRAFV600E突变状态仍然是独立的预后因素。一致性指数从仅TNM模型的0.61 - 0.68增加到添加分子标志物的模型中的0.63 - 0.71,包含临床病理特征的模型中为0.65 - 0.73,包含所有协变量的模型中为0.66 - 0.74。在具有完整注释的验证队列中,综合时间依赖性AUC从仅TNM模型的0.64增加到包含临床病理特征(无论有无分子标志物)的模型中的0.67。在接受辅助化疗的患者队列中,TNM、临床病理特征和分子标志物解释的方差相对比例平均分别为65%、25%和10%。
将MSI、BRAFV600E和KRAS突变状态纳入TNM分期的总生存模型中,可提高对II期和III期CC患者进行精确预后预测的能力,但在包含临床病理特征的多变量模型中,尤其是在接受化疗的患者中,预测准确性仅适度提高。