Department of Medical Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Translational Oncology, Pfizer, San Diego, CA, USA.
Nat Med. 2020 Nov;26(11):1733-1741. doi: 10.1038/s41591-020-1044-8. Epub 2020 Sep 7.
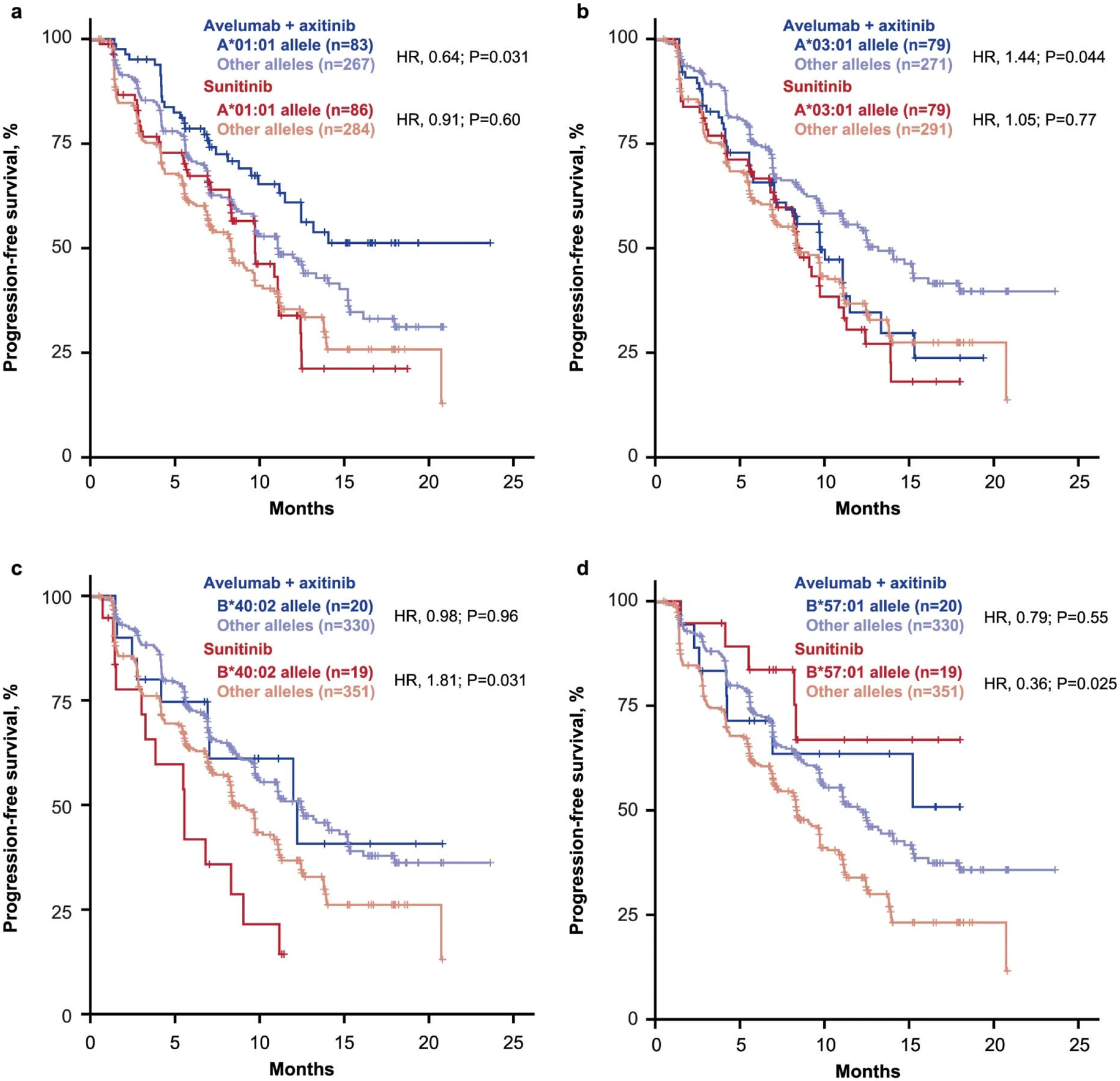
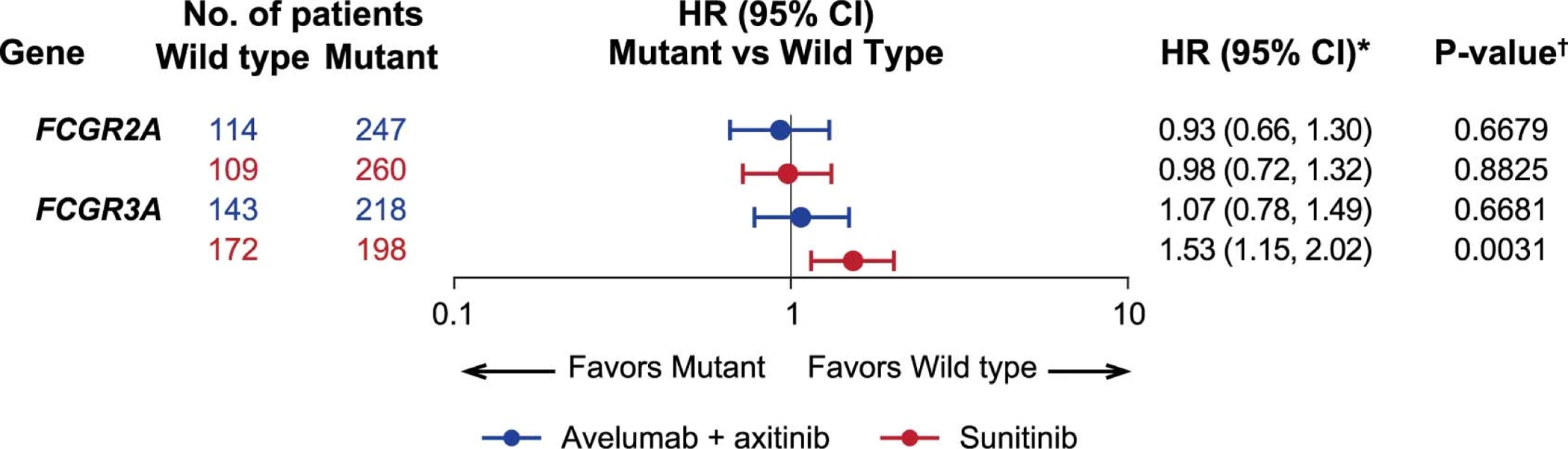
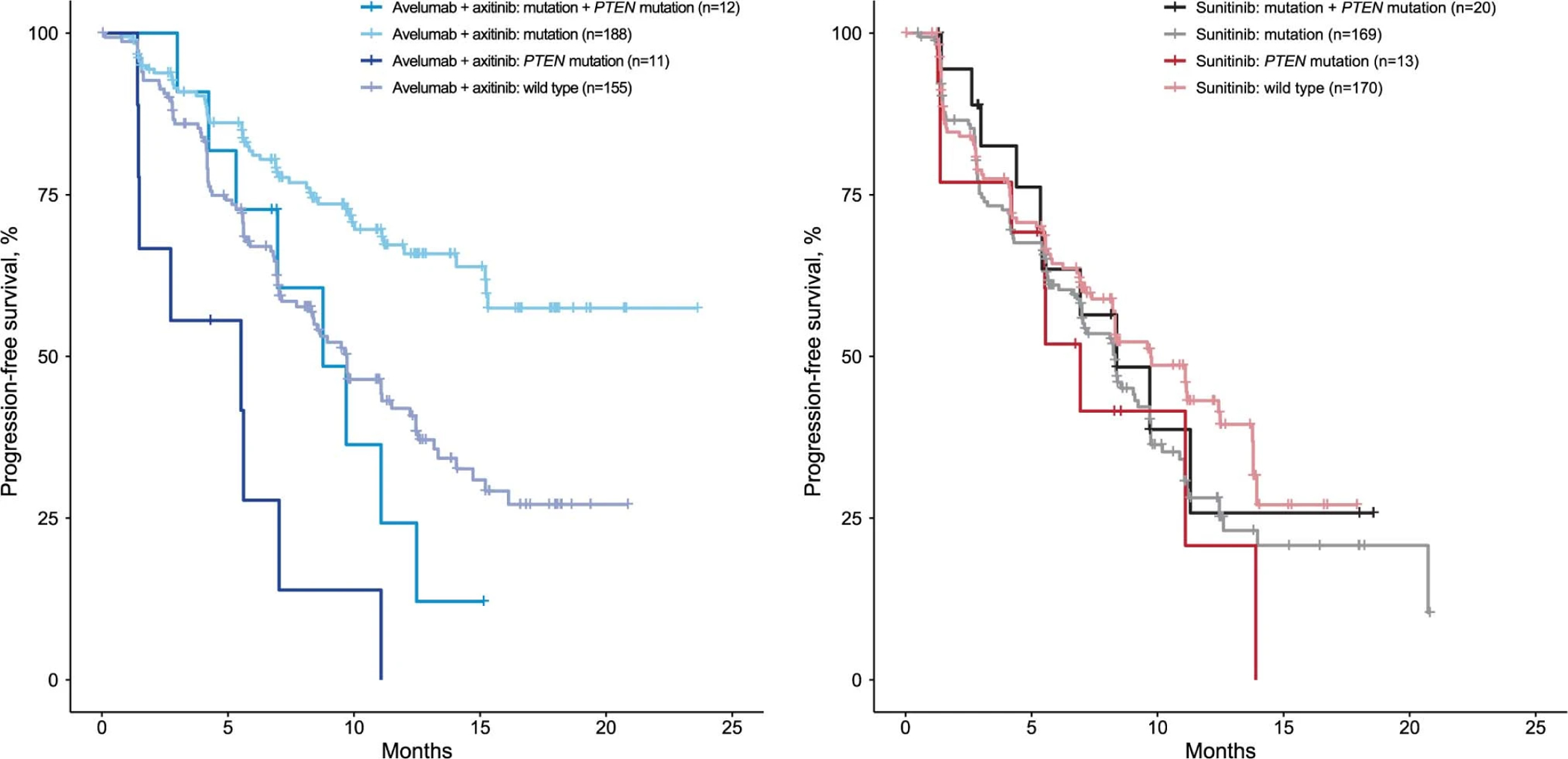
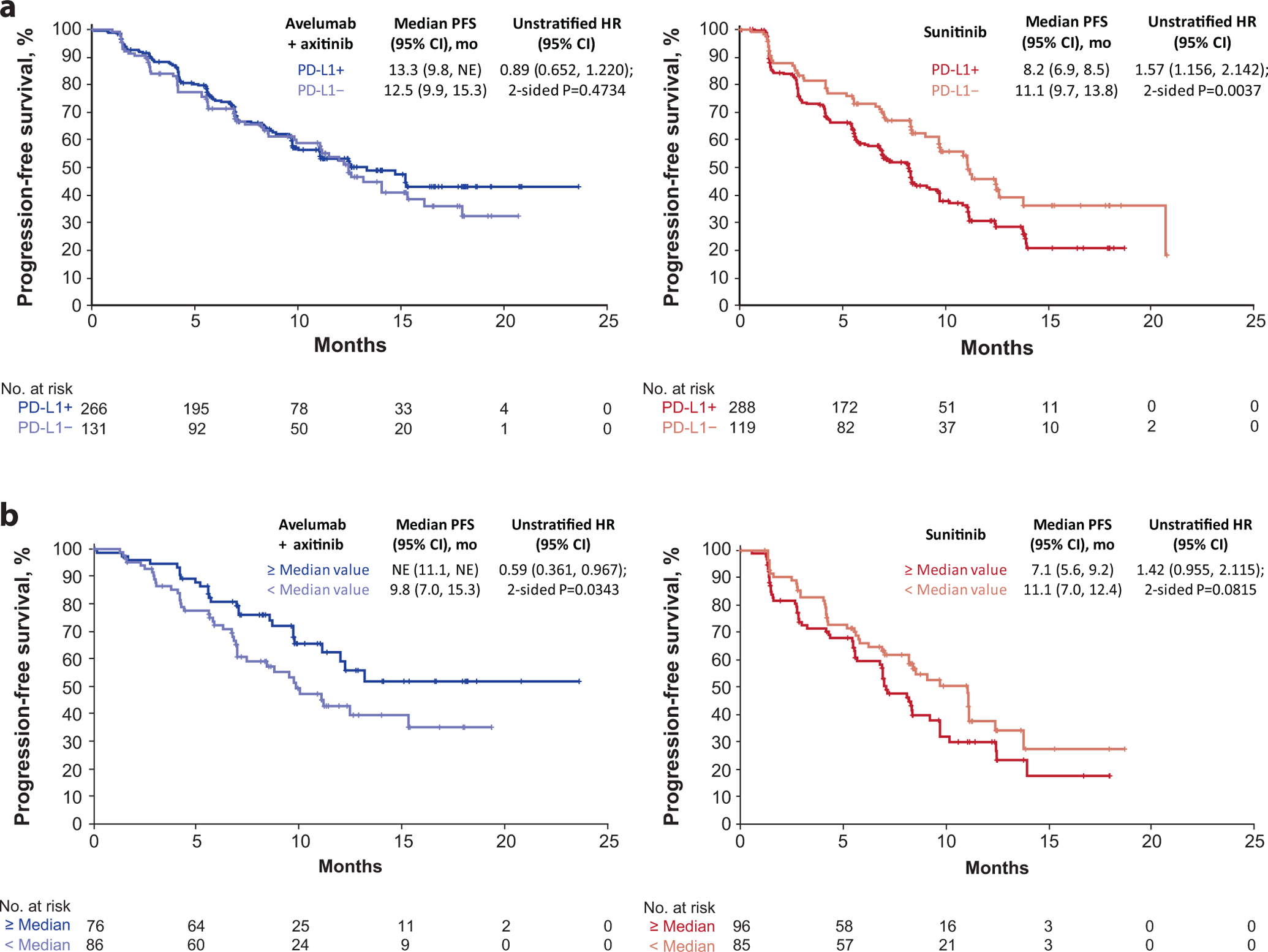
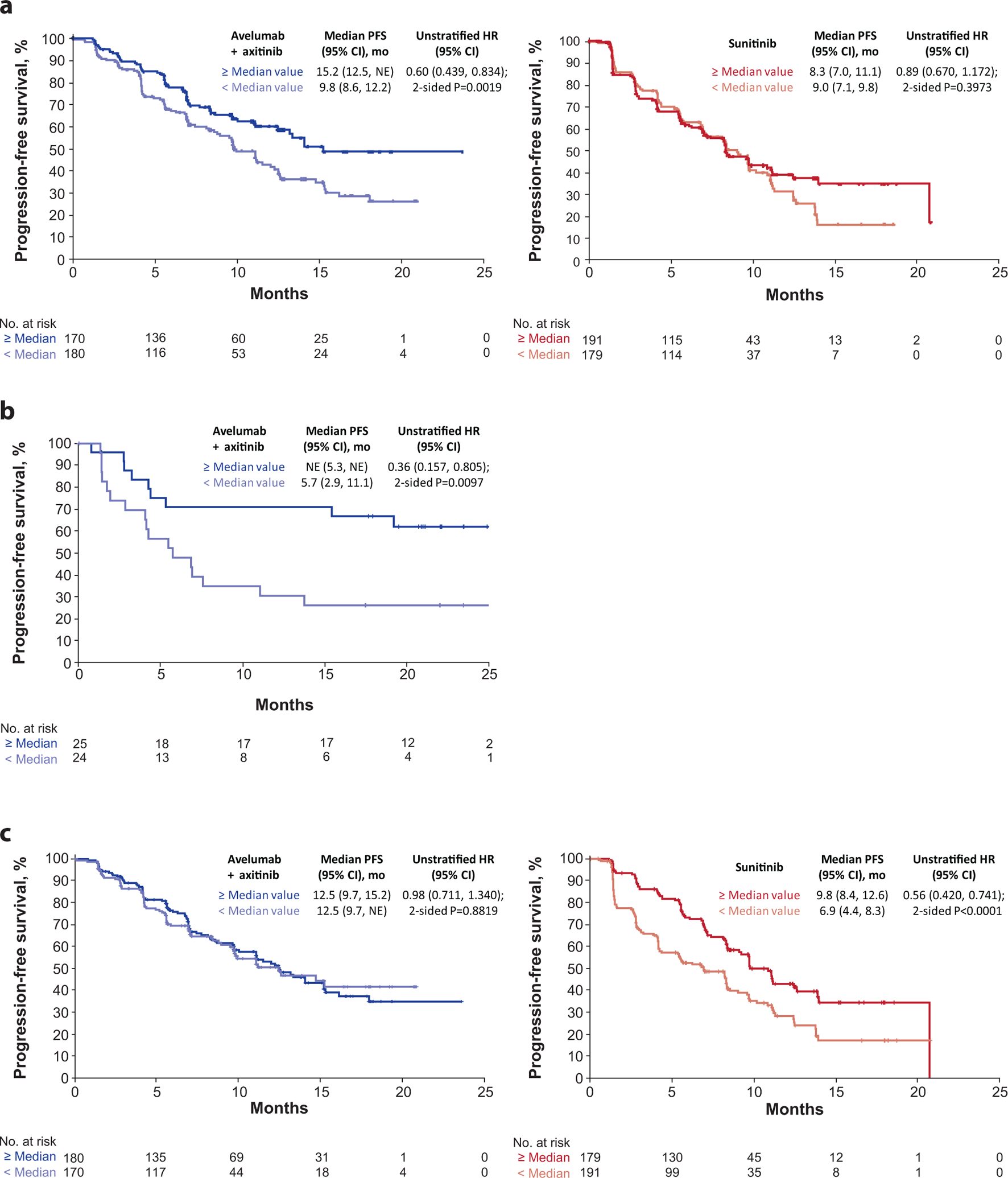
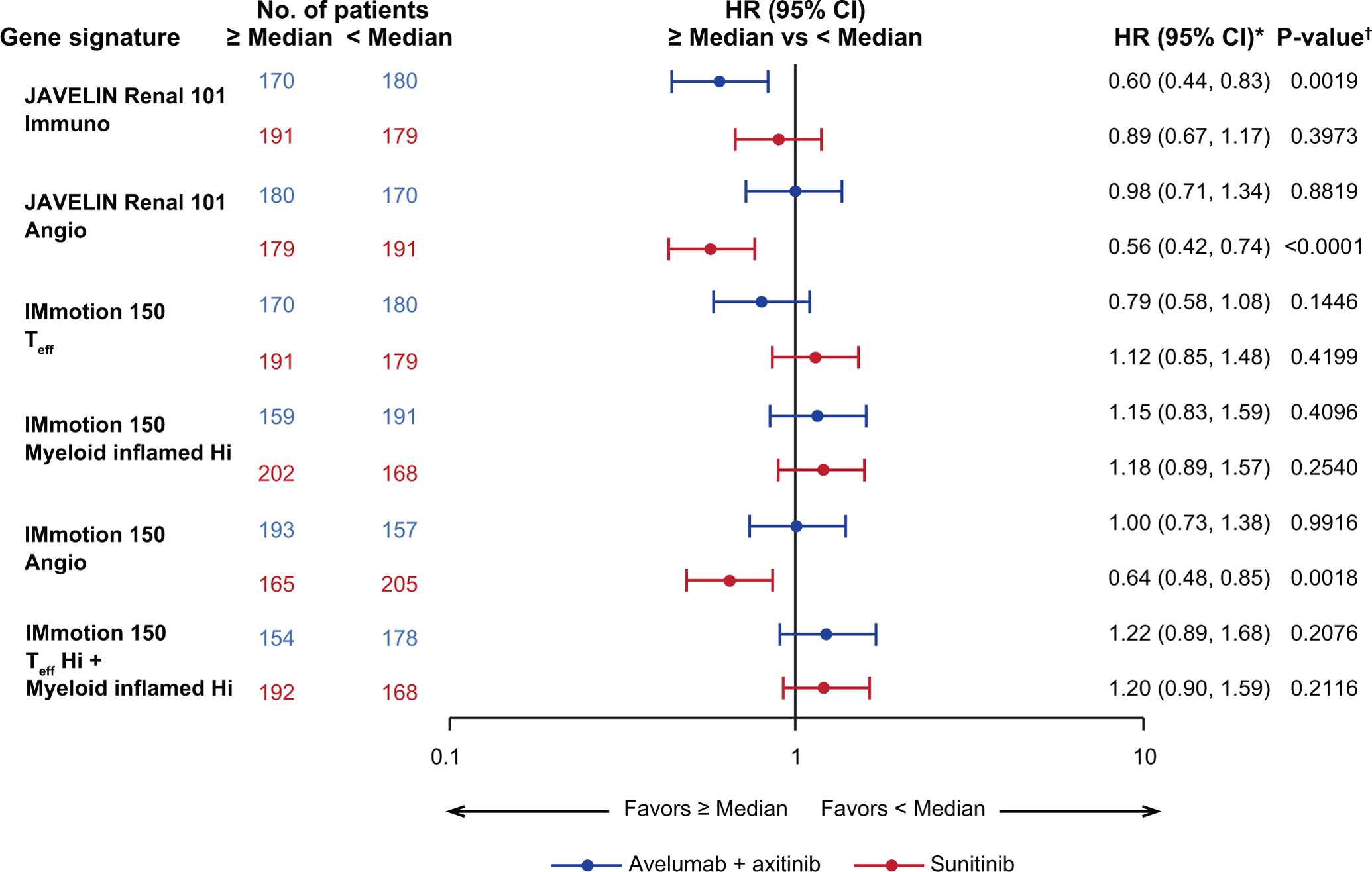
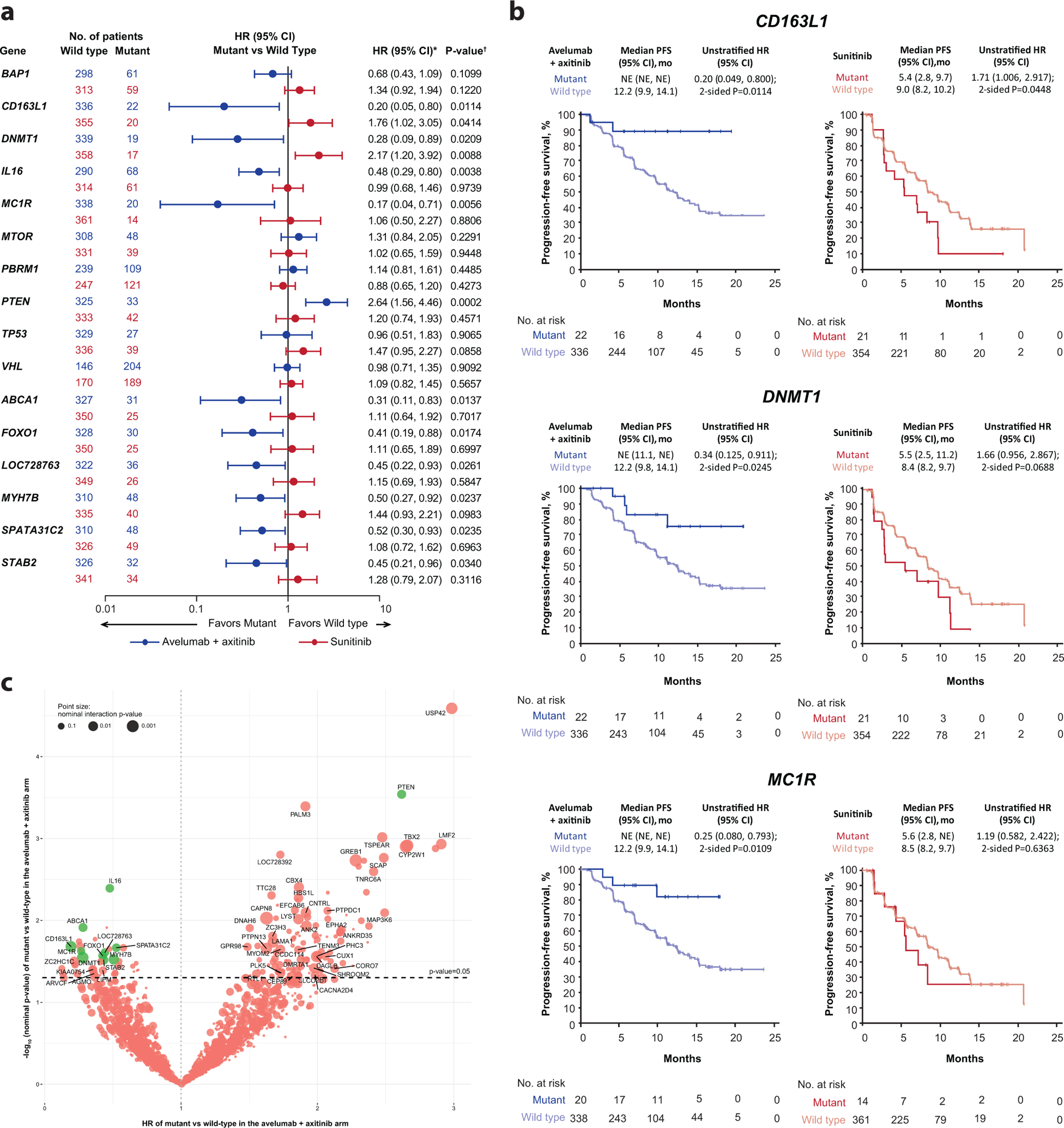
We report on molecular analyses of baseline tumor samples from the phase 3 JAVELIN Renal 101 trial (n = 886; NCT02684006 ), which demonstrated significantly prolonged progression-free survival (PFS) with first-line avelumab + axitinib versus sunitinib in advanced renal cell carcinoma (aRCC). We found that neither expression of the commonly assessed biomarker programmed cell death ligand 1 (PD-L1) nor tumor mutational burden differentiated PFS in either study arm. Similarly, the presence of FcɣR single nucleotide polymorphisms was unimpactful. We identified important biological features associated with differential PFS between the treatment arms, including new immunomodulatory and angiogenesis gene expression signatures (GESs), previously undescribed mutational profiles and their corresponding GESs, and several HLA types. These findings provide insight into the determinants of response to combined PD-1/PD-L1 and angiogenic pathway inhibition and may aid in the development of strategies for improved patient care in aRCC.
我们报告了 3 期 JAVELIN Renal 101 试验(n=886;NCT02684006)基线肿瘤样本的分子分析结果,该试验表明,在晚期肾细胞癌(aRCC)中,一线avelumab+axitinib 与舒尼替尼相比,显著延长了无进展生存期(PFS)。我们发现,无论是常见的生物标志物程序性死亡配体 1(PD-L1)的表达,还是肿瘤突变负担,都不能区分两个研究臂的 PFS。同样,FcɣR 单核苷酸多态性的存在也没有影响。我们确定了与治疗臂之间 PFS 差异相关的重要生物学特征,包括新的免疫调节和血管生成基因表达谱(GES)、以前未描述的突变谱及其相应的 GES 以及几种 HLA 类型。这些发现为联合 PD-1/PD-L1 和血管生成通路抑制反应的决定因素提供了深入了解,并可能有助于制定改善 aRCC 患者治疗的策略。