Yonsei University, Wonju, Republic of Korea.
JMIR Mhealth Uhealth. 2020 Sep 8;8(9):e20848. doi: 10.2196/20848.
In Ethiopia, health extension workers (HEWs) are deployed across the country by the government to meet public health needs. Team communication is important for effective teamwork, but community health workers in low-resource settings like Ethiopia may face challenges in carrying out team meetings to compile service statistics. This is due to the nature of their outreach activities, which requires extensive travel.
This study aimed to identify gaps in team communication about service statistics among HEWs in Ethiopia. Considering mobile communication and data collection as tools for bridging these gaps, we examined disparities in access to electricity, which has been identified as one of the major barriers to this approach.
Data from the most recent Performance Monitoring and Accountability 2020 service delivery point survey were used for our analysis. Logistic regression analysis was performed to identify disparities in team communication on service statistics for family planning, which is a major component of the HEW's job. Disparities were examined across health facilities with different levels of HEW integration in their staffing structure (ie, no HEWs, at least one HEW, or only HEWs). Additionally, a chi-square test was conducted to examine disparities in access to electricity to explore the potential of mobile communication and data collection integration.
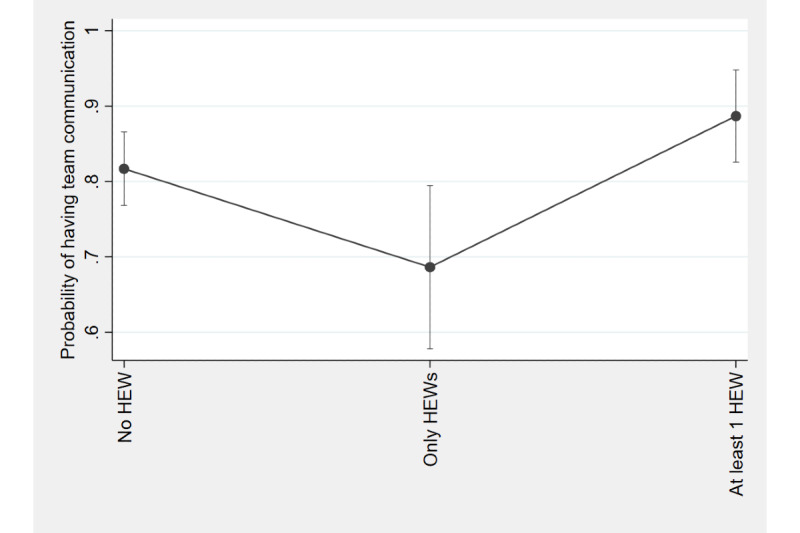
In total, 427 health facilities of four different types (ie, hospitals, health centers, health posts, and health clinics) were included in our analysis. At most health posts (84/95, 88%), only HEWs were employed; none of the health clinics integrated the HEW model into their staffing structure. Among the 84 health posts, the odds of having team meetings on family planning service statistics in the past 12 months were 0.48 times the odds of those without HEWs (P=.02). No statistically significant differences were found between HEW-only facilities and facilities with at least one HEW. Most health facilities (69/83, 83.13%) with HEWs as the only staff had no electricity at the time of the survey while 71.25% (57/80) had intermittent access (ie, service disruption lasting 2 or more hours that day). There were statistically significant differences in electricity access among health facilities with different levels of HEW integration (P<.001).
Facilities employing only HEWs were less likely to have regular team meetings to discuss service statistics. Since their responsibilities involve extensive outreach activities, travel, and paper-based recordkeeping, empowering HEWs with mobile communication and data collection can be a workable solution. The empirical evidence regarding disparities in electricity access also supports the need for and the feasibility of this approach.
在埃塞俄比亚,政府部署了卫生推广员(HEWs)在全国各地满足公共卫生需求。团队沟通对于有效的团队合作很重要,但像埃塞俄比亚这样资源匮乏环境中的社区卫生工作者在开展团队会议以编制服务统计数据时可能会面临挑战。这是由于他们的外展活动性质所致,这些活动需要大量的旅行。
本研究旨在确定埃塞俄比亚 HEW 之间关于服务统计数据的团队沟通中的差距。考虑到移动通信和数据收集是弥合这些差距的工具,我们研究了电力获取方面的差异,这被认为是该方法的主要障碍之一。
本研究使用了最近的 2020 年绩效监测和问责制服务提供点调查的数据进行分析。使用逻辑回归分析来确定计划生育服务统计数据方面的团队沟通差距,计划生育是 HEW 工作的主要组成部分之一。根据 HEW 在人员配备结构中的整合程度(即无 HEW、至少有一名 HEW 或只有 HEW),在不同类型的卫生设施中检查了差异。此外,还进行了卡方检验,以探讨获取电力的差异,探索移动通信和数据收集整合的潜力。
总共纳入了 427 个不同类型的卫生设施(即医院、卫生中心、卫生所和卫生诊所)进行分析。在大多数卫生所(84/95,88%)中,仅雇用 HEW;没有一个卫生诊所将 HEW 模式纳入其人员配备结构。在 84 个卫生所中,过去 12 个月内举行计划生育服务统计数据团队会议的几率是没有 HEW 的几率的 0.48 倍(P=.02)。仅 HEW 设施和至少有一名 HEW 的设施之间没有统计学上的显著差异。大多数拥有 HEW 作为唯一员工的卫生设施(83.13%,69/83)在调查时没有电力,而 71.25%(57/80)间歇性供电(即当天服务中断持续 2 小时或更长时间)。在 HEW 整合程度不同的卫生设施中,电力供应存在统计学上的显著差异(P<.001)。
仅雇用 HEW 的设施不太可能定期举行团队会议讨论服务统计数据。由于他们的职责涉及广泛的外展活动、旅行和基于纸张的记录保存,为 HEW 提供移动通信和数据收集工具可能是一种可行的解决方案。关于电力获取方面的差异的实证证据也支持这种方法的必要性和可行性。