Division of Nephrology, Department of Medicine, University of California, San Francisco.
Division of Pediatric Nephrology, Department of Pediatrics, University of California, San Francisco.
JAMA Netw Open. 2020 Sep 1;3(9):e2016197. doi: 10.1001/jamanetworkopen.2020.16197.
Survival of patients receiving dialysis has improved during the last 2 decades. However, few studies have examined temporal trends in the attributed causes of death (especially cardiovascular-related) in young populations.
To determine temporal trends and risk of cause-specific mortality (ie, cardiovascular and infectious) for children and young adults receiving dialysis.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study examined the records of children and young adults (aged <30 years) starting dialysis between 1995 and 2015 according to the United States Renal Data System database. Analyses were performed between June 2019 and June 2020. Fine-Gray models were used to examine trends in risk of different cardiovascular-related deaths. Models were adjusted for age, sex, race, neighborhood income, cause of end-stage kidney disease, insurance type, and comorbidities. Analyses were performed separately for children (ie, age <18 years) and young adults (between ages 18 and 30 years). Follow-up was censored at death or administratively, and transplantation was treated as a competing event.
Calendar year.
Cardiovascular cause-specific mortality.
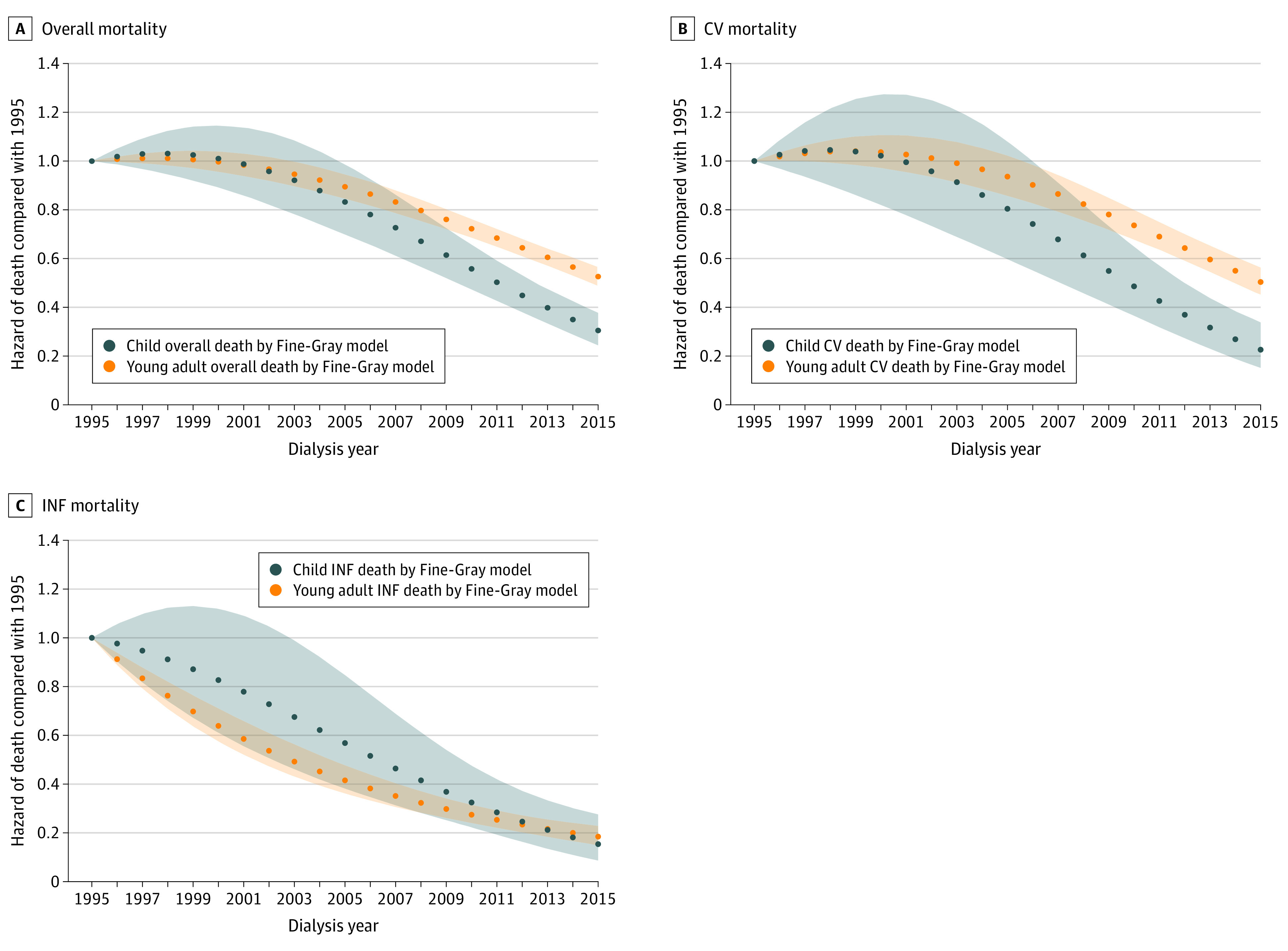
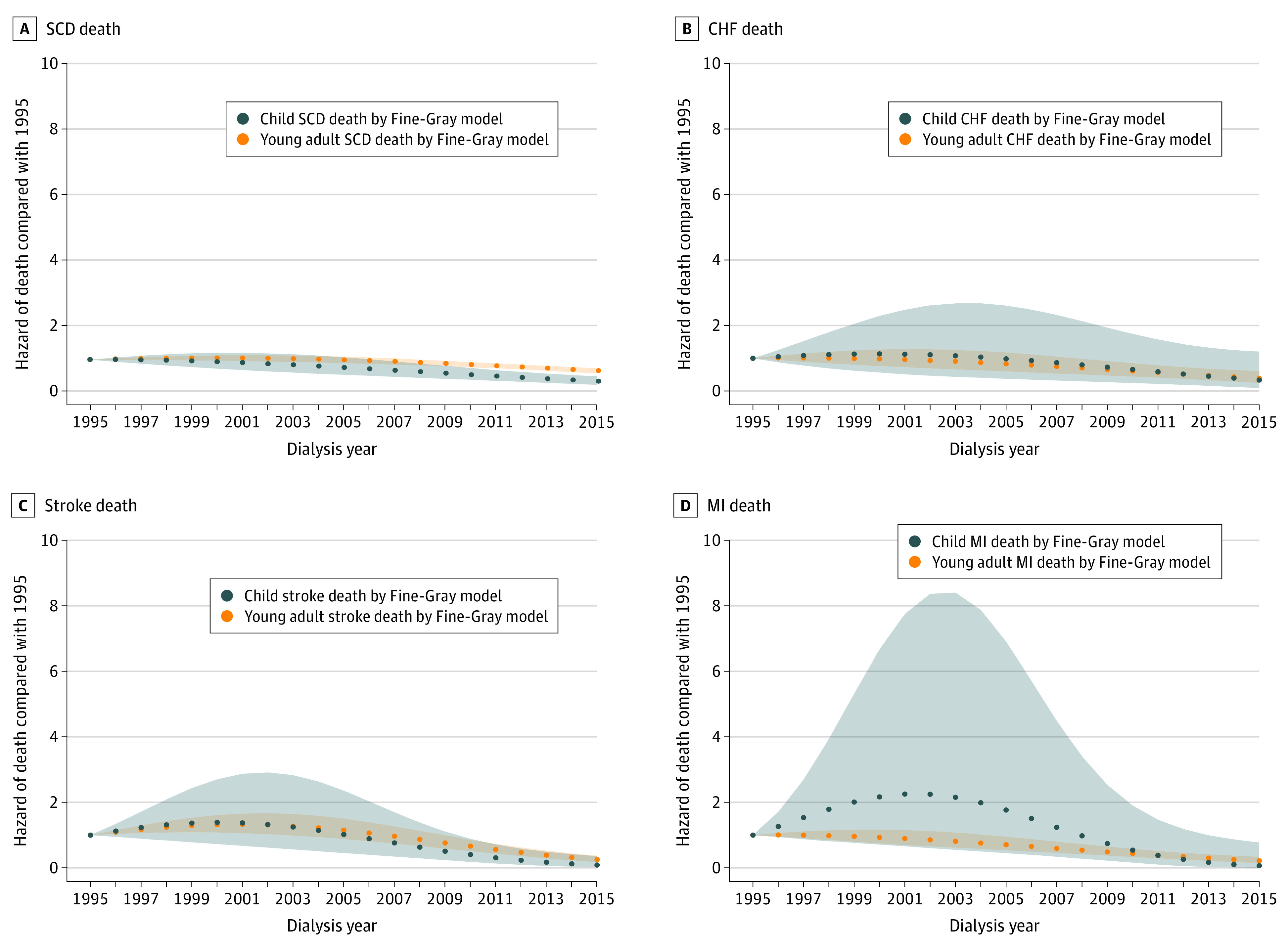
A total of 80 189 individuals (median [interquartile range] age, 24 [19-28] years; 36 259 [45.2%] female, 29 508 [36.8%] Black, and 15 516 [19.3%] Hispanic white) started dialysis and 16 179 experienced death during a median (interquartile range) of 14.3 (14.0-14.7) years of follow-up. Overall, 40.2% of deaths were from cardiovascular-related causes (6505 of 16 179 patients). In adjusted analysis, risk of cardiovascular-related death was stable initially but became statistically significantly lower after 2006 (vs 1995) in those starting dialysis as either children (subhazard ratio [SHR], 0.74; 95% CI, 0.55-1.00) or adults (SHR, 0.90; 95% CI, 0.83-0.98). Risk of sudden cardiac death improved steadily for all age groups, but to a greater degree in children (SHR, 0.31; 95% CI, 0.20-0.47) vs young adults (SHR, 0.64; 95% CI, 0.56-0.73) comparing 2015 vs 1995. Risk of stroke became statistically significantly lower around 2010 (vs 1995) for children (SHR, 0.40; 95% CI, 0.18-0.88) and young adults (SHR, 0.76; 95% CI, 0.59-0.99).
In this study, the risk of cardiovascular-related death declined for children and young adults starting dialysis during the last 2 decades, but trends differed depending on age at dialysis initiation and the specific cause of death. Additional studies are needed to improve risk of cardiovascular disease in young populations.
在过去的二十年中,接受透析治疗的患者的生存率得到了提高。然而,很少有研究调查年轻人群中归因于死亡的原因(尤其是心血管相关原因)的时间趋势。
确定接受透析的儿童和青年患者的特定原因死亡率(即心血管和传染性)的时间趋势和风险。
设计、设置和参与者:本回顾性队列研究根据美国肾脏数据系统数据库,对 1995 年至 2015 年期间开始透析的儿童和青年(年龄<30 岁)的记录进行了研究。分析于 2019 年 6 月至 2020 年 6 月之间进行。精细灰色模型用于检查不同心血管相关死亡风险的趋势。模型根据年龄、性别、种族、社区收入、终末期肾病的原因、保险类型和合并症进行了调整。分别对儿童(即年龄<18 岁)和青年(年龄在 18 至 30 岁之间)进行了分析。随访截止于死亡或行政,移植被视为竞争事件。
日历年份。
心血管原因的特定死亡率。
共有 80189 人(中位数[四分位间距]年龄,24 [19-28] 岁;36259 名[45.2%]女性,29508 名[36.8%]黑人,15516 名[19.3%]西班牙裔白人)开始透析,中位数(四分位间距)随访 14.3(14.0-14.7)年期间,有 16179 人经历了死亡。总体而言,40.2%的死亡是心血管相关原因(16179 名患者中的 6505 人)。在调整分析中,心血管相关死亡的风险最初是稳定的,但在 2006 年(与 1995 年相比)后,无论是儿童(亚危险比[SHR],0.74;95%CI,0.55-1.00)还是成人(SHR,0.90;95%CI,0.83-0.98)开始透析的患者中,该风险的统计学意义显著降低。所有年龄段的心脏性猝死风险均稳步改善,但儿童的改善程度更大(SHR,0.31;95%CI,0.20-0.47),而青年(SHR,0.64;95%CI,0.56-0.73)相比,2015 年与 1995 年相比。儿童(SHR,0.40;95%CI,0.18-0.88)和青年(SHR,0.76;95%CI,0.59-0.99)的中风风险在 2010 年左右统计学意义显著降低(与 1995 年相比)。
在这项研究中,在过去的二十年中,开始透析的儿童和青年的心血管相关死亡风险有所下降,但趋势因透析开始时的年龄和特定的死亡原因而异。需要进一步研究以改善年轻人群的心血管疾病风险。