Department of Orthopedic Surgery, Eulji University School of Medicine, Daejeon, Korea.
Clin Orthop Surg. 2020 Sep;12(3):353-363. doi: 10.4055/cios19126. Epub 2020 Jun 29.
The goal of this study was to evaluate the clinical and radiological outcomes of arthroscopic partial repair with medialization of the attachment site of the rotator cuff tendon and to identify prognostic factors affecting rotator cuff healing in patients with irreparable large to massive posterosuperior rotator cuff tears.
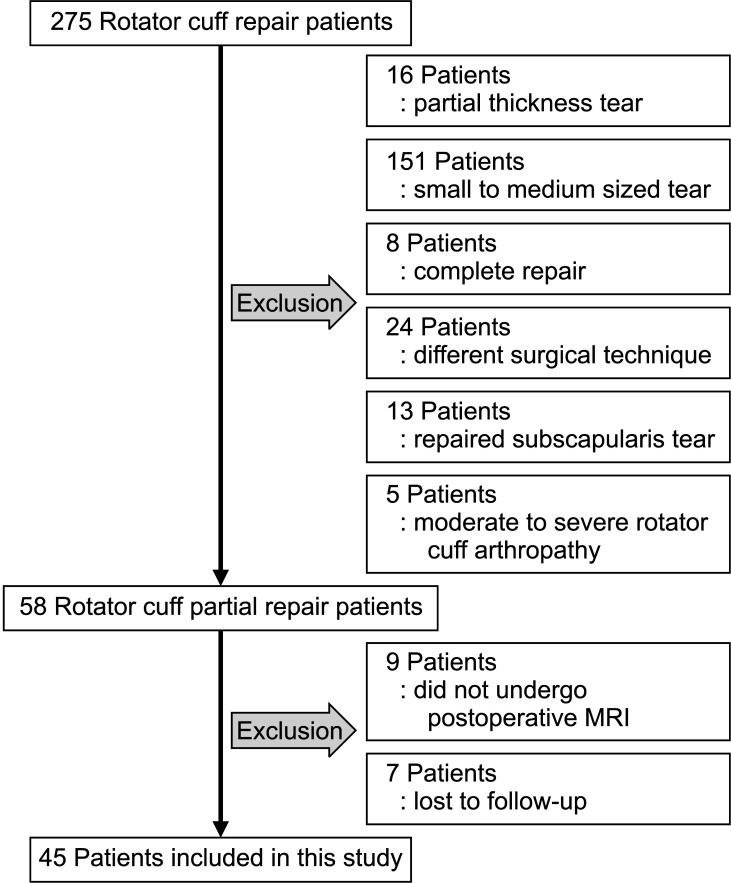
Between July 2012 and March 2016, 42 patients with irreparable large to massive posterosuperior rotator cuff tears underwent an arthroscopic partial repair with medialization of the attachment site of the rotator cuff tendon. All patients had a minimum of 2-year follow-up (mean, 35.4 ± 7.3 months). Clinical evaluation was performed using the visual analog scale, the University of California, Los Angeles shoulder rating scale, Constant score, and active range of motion. Radiological evaluation was performed using magnetic resonance imaging and simple radiography.
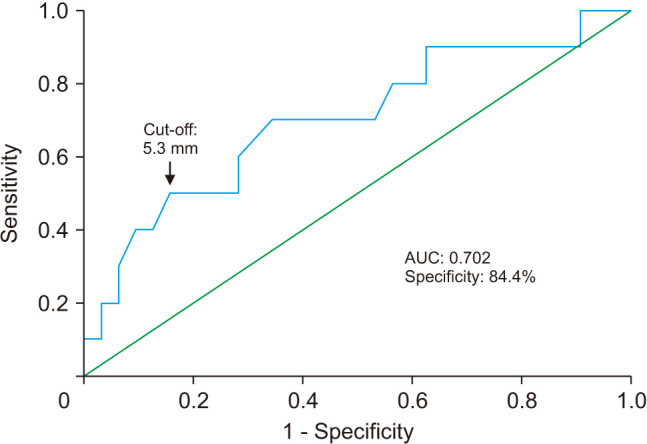
Clinical outcomes at the final follow-up improved significantly compared with the preoperative values (all < 0.001). The failure rate was 23.8% (10/42); however, clinical outcomes significantly improved regardless of cuff healing (all < 0.001). The mean acromiohumeral distance was 6.5 ± 1.7 mm (range, 3.2-9.7 mm) before surgery and 6.3 ± 1.6 mm (range, 2.8-9.5 mm) at the final follow-up. Preoperative acromiohumeral distance was associated with failure of cuff healing in the univariate analysis ( = 0.043) and multivariate analysis ( = 0.048). A receiver operating characteristic curve was used to determine the predictive cutoff value for the smallest preoperative acromiohumeral distance for successful healing, which was calculated as 5.3 mm.
Despite healing failure, arthroscopic partial repair with medialization can be a possible treatment option for irreparable large to massive posterosuperior rotator cuff tears because of the improvement in clinical outcome. The shorter preoperative acromiohumeral distance was the single most important factor negatively affecting cuff healing, and the likelihood of success of healing might be improved if a repair is performed when the preoperative acromiohumeral distance is < 5.3 mm.
本研究的目的是评估关节镜下部分修复合并冈上肌腱附着点内侧化治疗不可修复的巨大或巨大肩袖后上侧撕裂的临床和影像学结果,并确定影响不可修复的巨大或巨大肩袖后上侧撕裂患者肩袖愈合的预后因素。
2012 年 7 月至 2016 年 3 月,42 例不可修复的巨大或巨大肩袖后上侧撕裂患者接受了关节镜下部分修复合并冈上肌腱附着点内侧化。所有患者均获得至少 2 年的随访(平均 35.4 ± 7.3 个月)。临床评估采用视觉模拟评分、加利福尼亚大学洛杉矶分校肩关节评分、Constant 评分和主动活动范围。影像学评估采用磁共振成像和简单的 X 线摄影。
与术前相比,最终随访时的临床结果显著改善(均<0.001)。失败率为 23.8%(10/42);然而,无论肩袖愈合情况如何,临床结果均显著改善(均<0.001)。手术前肩峰肱骨头间距平均值为 6.5 ± 1.7mm(范围,3.2-9.7mm),最终随访时为 6.3 ± 1.6mm(范围,2.8-9.5mm)。单因素分析和多因素分析均显示术前肩峰肱骨头间距与肩袖愈合失败相关(=0.043,=0.048)。受试者工作特征曲线用于确定成功愈合的最小术前肩峰肱骨头间距的预测临界值,计算结果为 5.3mm。
尽管存在愈合失败,但关节镜下部分修复合并冈上肌腱附着点内侧化仍可能是不可修复的巨大或巨大肩袖后上侧撕裂的一种治疗选择,因为临床结果得到了改善。较短的术前肩峰肱骨头间距是影响肩袖愈合的最重要的单一负面因素,如果在术前肩峰肱骨头间距<5.3mm 时进行修复,愈合的成功率可能会提高。