Serag Waleed Mohamed, Mohammed Bedoor Shehap Eldeen, Mohamed Magdy Mahmoud, Elsayed Basem Eysa
Department of Chemistry, Faculty of Science, Suez University, Suez, Egypt.
Chemical Administration, Suez, Egypt.
Heliyon. 2020 Aug 20;6(8):e04677. doi: 10.1016/j.heliyon.2020.e04677. eCollection 2020 Aug.
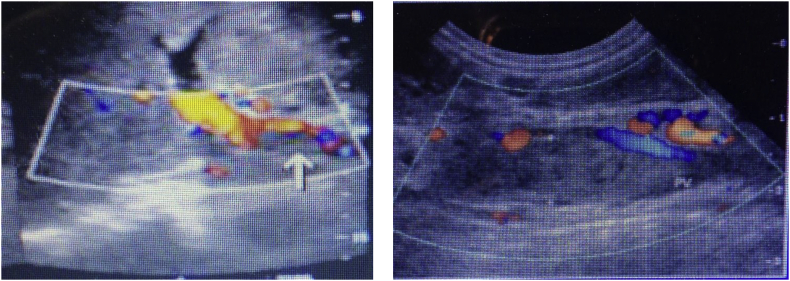
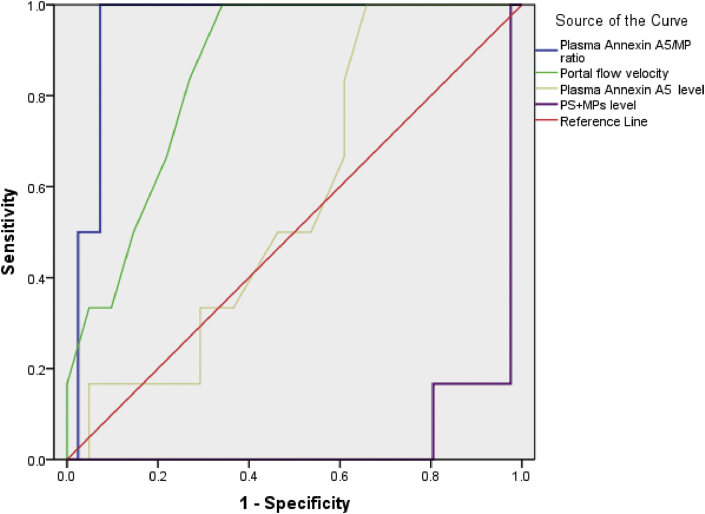
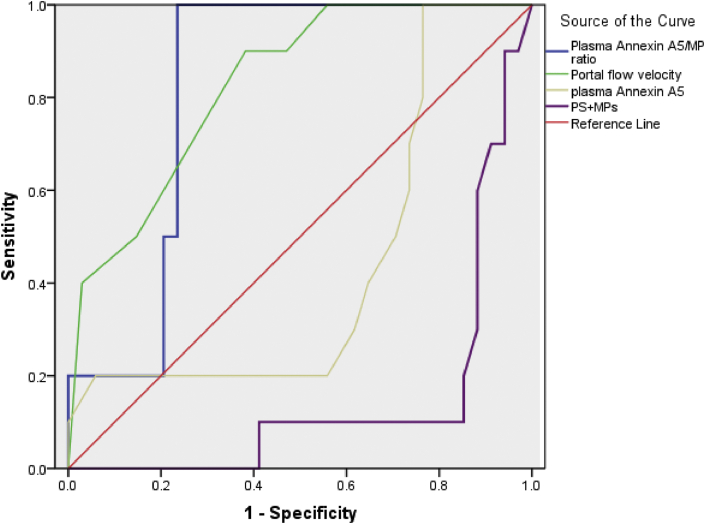
The mechanisms of the hypercoagulable state in cirrhotics with and without hepatocellular carcinoma are incompetently comprehended. Objective: We aimed to explore the plasma Annexin A5/PS + MP ratio in these patients. Higher levels of Annexin A5 and PhosphatidylSerine bearing microparticles have been observed in cases of inflammation and increased coagulation but there are no studies which explore if there is an association between them and PVT in cirrhotics with and without HCC. So, our goal is to estimate their role in predicting PVT within HCV cirrhotics with and without HCC. 91 HCV cirrhotics with and without HCC and 20 healthy people (controls) were enlisted. Cirrhotics with and without HCC who developed PVT displayed higher levels of PS + MPs and lower Annexin A5/PS + MPs ratio (38.73 ± 1.92) and (0.00238 ± 0.00047) than cirrhotics who didn't develop PVT (22.19 ± 10.58) and (0.00451 ± 0.0023) (P < 0.001). Among the tested factors, lower Annexin A5/PS + MPs ratio show higher performance in predicting PVT in total cirrhotics, AUC, 0.919 followed by PS + MPs level, 0.876, Portal flow velocity, 0.842, Plasma Annexin A5 level, 0.509. In our hypothesis, As phosphatidylserine exposure increase due to increased level of circulating microparticles in cirrhotics with and without HCC, anenxin-A5 may be secreted by platelets and endothelial cells into the circulation as a physiological response to inactivate the elevated levels of PS bearing MPs produced in these patients but the increase in anenxin-A5 level isn't equivalent to the increase in PS bearing MPs levels. The equilibrium between plasma annexin A5 and PS bearing MPs levels is defected.
肝硬化合并或不合并肝细胞癌患者高凝状态的机制尚未完全明了。目的:我们旨在探究这些患者血浆中膜联蛋白A5/磷脂酰丝氨酸阳性微颗粒(Annexin A5/PS + MP)的比例。在炎症和凝血增强的病例中已观察到较高水平的膜联蛋白A5和携带磷脂酰丝氨酸的微颗粒,但尚无研究探讨它们与肝硬化合并或不合并肝细胞癌患者门静脉血栓形成(PVT)之间是否存在关联。因此,我们的目标是评估它们在预测合并或不合并肝细胞癌的丙型肝炎病毒(HCV)肝硬化患者发生PVT中的作用。招募了91例合并或不合并肝细胞癌的HCV肝硬化患者以及20名健康人(对照组)。发生PVT的合并或不合并肝细胞癌的肝硬化患者,其PS + MPs水平较高,而Annexin A5/PS + MPs比例较低(分别为38.73±1.92和0.00238±0.00047),低于未发生PVT的肝硬化患者(分别为22.19±10.58和0.00451±0.0023)(P<0.001)。在所有检测因素中,较低的Annexin A5/PS + MPs比例在预测总体肝硬化患者发生PVT方面表现更佳,曲线下面积(AUC)为0.919,其次是PS + MPs水平,为0.876,门静脉血流速度为0.842,血浆膜联蛋白A5水平为0.509。在我们的假设中,由于合并或不合并肝细胞癌的肝硬化患者循环微颗粒水平升高导致磷脂酰丝氨酸暴露增加,血小板和内皮细胞可能会分泌膜联蛋白A5进入循环,作为一种生理反应来灭活这些患者体内产生的升高水平的携带PS的微颗粒,但膜联蛋白A5水平的升高并不等同于携带PS的微颗粒水平的升高。血浆膜联蛋白A5与携带PS的微颗粒水平之间的平衡被打破。