Wennmann Markus, Hielscher Thomas, Kintzelé Laurent, Menze Bjoern H, Langs Georg, Merz Maximilian, Sauer Sandra, Kauczor Hans-Ulrich, Schlemmer Heinz-Peter, Delorme Stefan, Goldschmidt Hartmut, Weinhold Niels, Hillengass Jens, Weber Marc-André
Division of Radiology, German Cancer Research Center (DKFZ), Im Neuenheimer Feld 280, 69120 Heidelberg, Germany.
Diagnostic and Interventional Radiology, University Hospital Heidelberg, Im Neuenheimer Feld 110, 69120 Heidelberg, Germany.
Cancers (Basel). 2020 Sep 7;12(9):2537. doi: 10.3390/cancers12092537.
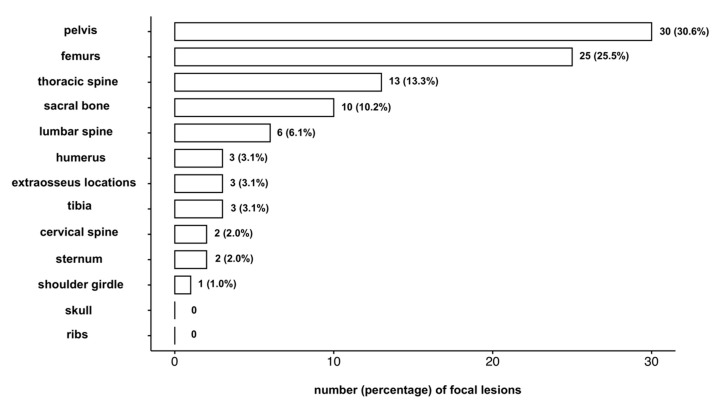
The purpose of this study was to assess how different MRI protocols (spinal vs. spinal plus pelvic vs. whole-body (wb)-MRI) affect staging in patients with smoldering multiple myeloma (SMM), according to the SLiM-CRAB-criterion '>1 focal lesion (FL) in MRI'. In this retrospective study, a baseline cohort of 147 SMM patients with wb-MRI at initial diagnosis was investigated, including prognostic data regarding development of CRAB-criteria. Fifty-two patients formed a follow-up cohort with a median of three wb-MRIs. The locations of all FLs were determined and it was calculated how staging decisions regarding the criterion '>1 FL in MRI' would have been made if only a limited anatomic area (spine vs. spine plus pelvis) would have been covered by the MRI protocol. Furthermore, subgroups of patients selected by different cutoff-protocol-combinations were compared regarding their prognosis for development of CRAB-criteria. With an MRI protocol limited to spine/spine plus pelvis, only 28%/64% of patients who actually had >1 FL in wb-MRI would have been rated correctly as having '>1 FL in MRI'. Fifty-four percent/36% of patients with exactly 1 FL in spine/spine plus pelvis revealed >1 FL when the entire wb-MRI was analyzed. During follow-up, four more patients developed >1 FL in wb-MRI; both limited MRI protocols would have detected only one of these four patients as having >1 FL at the correct timepoint. Having >1 FL in spine/in spine plus pelvis/in the whole body was associated with a 43%/57%/49% probability of developing CRAB-criteria within 2 years. Patients with >3 FL in spine plus pelvis and patients with >4 FL in the whole body had an 80% probability to develop CRAB-criteria within 2 years. MRI protocols limited to the spine or to spine plus pelvis lead to substantial underdiagnoses of patients who actually have >1 FL in wb-MRI at baseline and during follow-up, which influences staging and treatment decisions according to the current SLiM-CRAB criteria. However, given the spatial distribution of FLs and the analysis on clinical course of patients indicates that the cutoff for the number of FLs should be adopted according to the MRI protocol when using MRI for staging in SMM.
本研究的目的是根据SLiM-CRAB标准“MRI中>1个局灶性病变(FL)”,评估不同的MRI方案(脊柱MRI、脊柱加骨盆MRI、全身(wb)-MRI)如何影响冒烟型多发性骨髓瘤(SMM)患者的分期。在这项回顾性研究中,对147例初诊时进行了全身MRI的SMM患者的基线队列进行了调查,包括与CRAB标准发展相关的预后数据。52例患者组成了一个随访队列,平均进行了三次全身MRI检查。确定了所有FL的位置,并计算了如果MRI方案仅覆盖有限的解剖区域(脊柱、脊柱加骨盆),关于“MRI中>1个FL”标准的分期决策会如何做出。此外,比较了根据不同的截止协议组合选择的患者亚组在CRAB标准发展方面的预后。当MRI方案仅限于脊柱/脊柱加骨盆时,在全身MRI中实际有>1个FL的患者中,只有28%/64%会被正确评定为“MRI中>1个FL”。在分析整个全身MRI时,脊柱/脊柱加骨盆中恰好有1个FL的患者中有54%/36%显示有>1个FL。在随访期间,又有4例患者在全身MRI中出现>1个FL;两种有限的MRI方案都只能在正确的时间点检测到这4例患者中的1例有>1个FL。脊柱/脊柱加骨盆/全身有>1个FL与2年内出现CRAB标准的概率分别为43%/57%/49%相关。脊柱加骨盆中有>3个FL和全身有>4个FL的患者在2年内出现CRAB标准的概率为80%。仅限于脊柱或脊柱加骨盆的MRI方案会导致对基线和随访期间全身MRI中实际有>1个FL的患者进行大量漏诊,这会影响根据当前SLiM-CRAB标准做出的分期和治疗决策。然而,考虑到FL的空间分布以及对患者临床病程的分析表明,在SMM分期中使用MRI时,应根据MRI方案采用FL数量的截止值。