Pellicori Pierpaolo, Ofstad Anne Pernille, Fitchett David, Zeller Cordula, Wanner Christoph, George Jyothis, Zinman Bernard, Brueckmann Martina, Lindenfeld JoAnn
Robertson Centre for Biostatistics, Glasgow Clinical Trials Unit, University of Glasgow, Glasgow, UK.
Boehringer Ingelheim Norway KS, Asker, Norway.
ESC Heart Fail. 2020 Dec;7(6):3401-3407. doi: 10.1002/ehf2.12891. Epub 2020 Sep 11.
The EMPA-REG OUTCOME trial demonstrated reductions in cardiovascular (CV) death and heart failure (HF) outcomes with empagliflozin, a sodium-glucose co-transporter 2 inhibitor, in patients with type 2 diabetes and established CV disease over a study period of 3 years. We aimed to investigate the early benefit-risk profile of empagliflozin in patients enrolled in the EMPA-REG OUTCOME trial according to HF status at baseline.
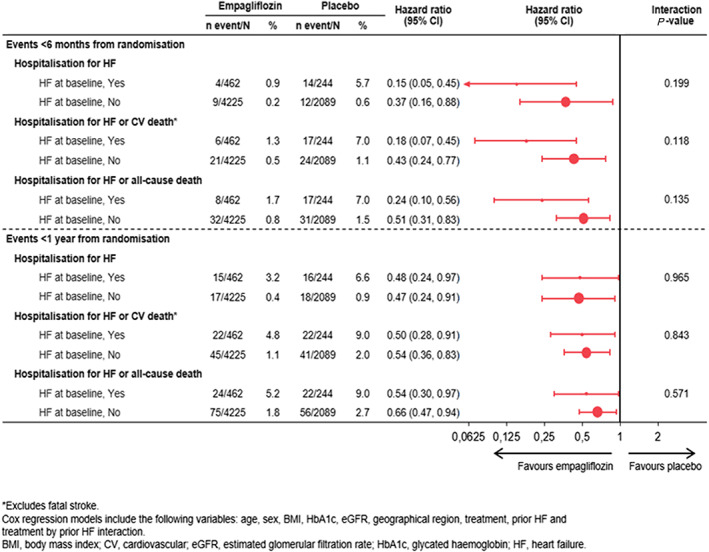
The effects of treatments on glycated haemoglobin, systolic blood pressure and body weight, and on the HF endpoints of hospitalization for HF (HHF), HHF or CV death, and HHF or all-cause mortality were evaluated at 12 weeks, 6 months, and 1 year after randomization. Occurrence of adverse events (AEs) during these time points was also evaluated. Compared with placebo, empagliflozin lowered glycated haemoglobin, systolic blood pressure, and body weight and rates of all the HF endpoints, as early as at 12 weeks, regardless of HF status at baseline. Favourable clinical and metabolic effects were maintained over time. AEs were generally higher in those with HF than without HF; however, compared with placebo, empagliflozin did not increase risk of developing AEs over the first year of treatment.
In the EMPA-REG OUTCOME trial, the use of empagliflozin led to early and beneficial effects on clinical, metabolic, and HF outcomes in patients with type 2 diabetes with or without HF at baseline, which were already apparent within 12 weeks from initiation of treatment. Over the first year of treatment, no safety concern was detected with the use of empagliflozin.
EMPA-REG OUTCOME试验表明,在为期3年的研究期间,钠-葡萄糖协同转运蛋白2抑制剂恩格列净可降低2型糖尿病合并已确诊心血管疾病患者的心血管(CV)死亡和心力衰竭(HF)风险。我们旨在根据基线时的HF状态,研究恩格列净在参与EMPA-REG OUTCOME试验患者中的早期获益-风险情况。
在随机分组后的12周、6个月和1年,评估治疗对糖化血红蛋白、收缩压和体重以及对HF住院(HHF)、HHF或CV死亡、HHF或全因死亡率等HF终点的影响。还评估了这些时间点不良事件(AE)的发生情况。与安慰剂相比,无论基线时的HF状态如何,恩格列净早在12周时就能降低糖化血红蛋白、收缩压和体重以及所有HF终点的发生率。随着时间推移,良好的临床和代谢效应得以维持。HF患者的AE总体上高于无HF患者;然而,与安慰剂相比,恩格列净在治疗的第一年并未增加发生AE的风险。
在EMPA-REG OUTCOME试验中,使用恩格列净对基线时有或无HF状态的2型糖尿病患者的临床、代谢和HF结局产生了早期有益影响,这些影响在开始治疗后的12周内就已明显显现。在治疗的第一年,未发现使用恩格列净存在安全问题。