Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, USA.
Massachusetts General Hospital Diabetes Center, Harvard Medical School, Boston, Massachusetts, USA.
Diabetes Obes Metab. 2022 Mar;24(3):442-454. doi: 10.1111/dom.14593. Epub 2021 Dec 1.
To investigate effectiveness and safety outcomes among patients with type 2 diabetes (T2D) initiating empagliflozin versus dipeptidyl peptidase-4 (DPP-4) inhibitor treatment across the broad spectrum of cardiovascular risk.
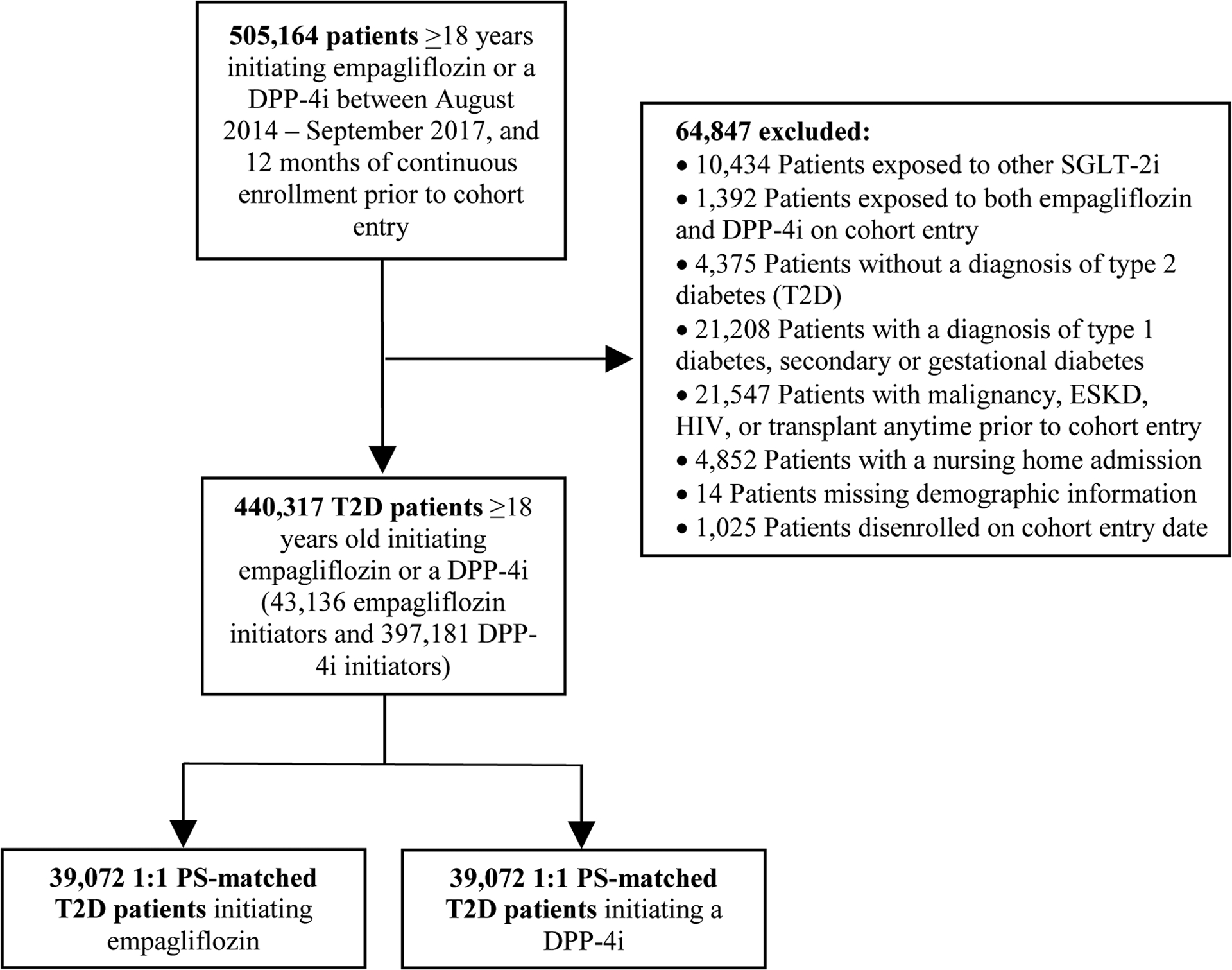
In a population-based cohort study we identified 39 072 pairs of 1:1 propensity score-matched adult patients with T2D initiating empagliflozin or DPP-4 inhibitors, using data from 2 US commercial insurance databases and Medicare between August 2014 and September 2017. The primary outcomes were a composite of myocardial infarction (MI)/stroke, and hospitalization for heart failure (HHF). Safety outcomes were bone fractures, lower-limb amputations (LLAs), diabetic ketoacidosis (DKA), and acute kidney injury (AKI). We estimated pooled hazard ratios (HRs) and 95% confidence intervals (CIs) adjusting for more than 140 baseline covariates.
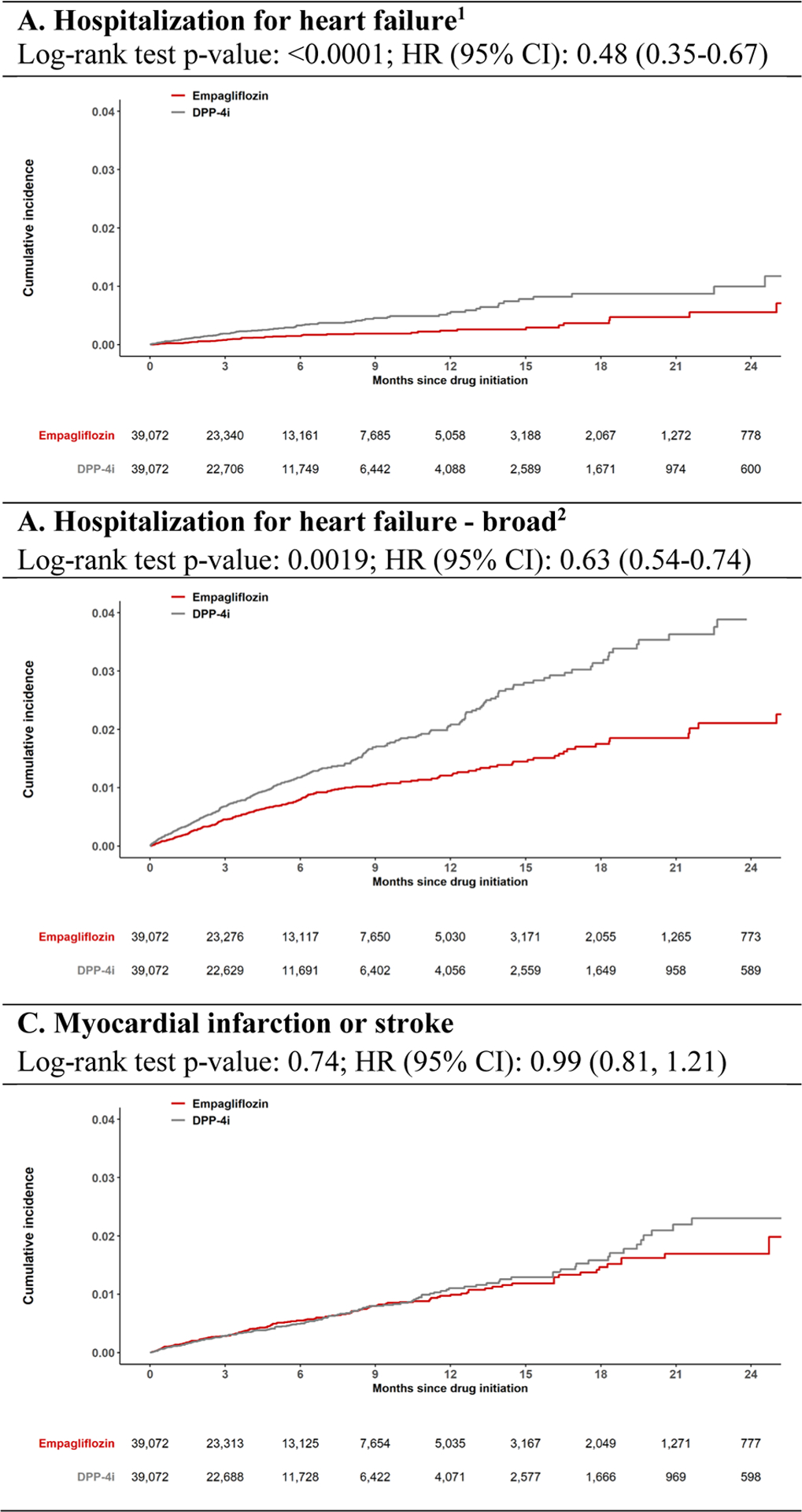
Study participants had a mean age of 60 years and only 28% had established cardiovascular disease. Compared to DPP-4 inhibitors, empagliflozin was associated with similar risk of MI/stroke (HR 0.99 [95% CI 0.81-1.21]), and lower risk of HHF (HR 0.48 [95% CI 0.35-0.67] and 0.63 [95% CI 0.54-0.74], based on a primary and any heart failure discharge diagnosis, respectively). The HR was 0.52 (95% CI 0.38-0.72) for all-cause mortality (ACM) and 0.83 (95% CI 0.70-0.98) for a composite of MI/stroke/ACM. Empagliflozin was associated with a similar risk of LLA and fractures, an increased risk of DKA (HR 1.71 [95% CI 1.08-2.71]) and a decreased risk of AKI (HR 0.60 [95% CI 0.43-0.85]).
In clinical practice, the initiation of empagliflozin versus a DPP-4 inhibitor was associated with a lower risk of HHF, ACM and MI/stroke/ACM, a similar risk of MI/stroke, and a safety profile consistent with documented information.
在广泛的心血管风险范围内,调查 2 型糖尿病(T2D)患者起始使用恩格列净与二肽基肽酶-4(DPP-4)抑制剂治疗的疗效和安全性结局。
在一项基于人群的队列研究中,我们使用来自美国 2 家商业保险数据库和 Medicare 在 2014 年 8 月至 2017 年 9 月间的数据,确定了 39072 对 1:1 倾向评分匹配的 T2D 成年患者,这些患者起始使用恩格列净或 DPP-4 抑制剂。主要结局为心肌梗死(MI)/卒中复合事件,以及心力衰竭住院(HHF)。安全性结局为骨折、下肢截肢(LLA)、糖尿病酮症酸中毒(DKA)和急性肾损伤(AKI)。我们估计了经 140 多项基线协变量调整后的合并风险比(HR)和 95%置信区间(CI)。
研究参与者的平均年龄为 60 岁,仅有 28%有明确的心血管疾病。与 DPP-4 抑制剂相比,恩格列净与 MI/卒中风险相似(HR 0.99 [95% CI 0.81-1.21]),而 HHF 风险较低(基于主要和任何心力衰竭出院诊断,HR 分别为 0.48 [95% CI 0.35-0.67]和 0.63 [95% CI 0.54-0.74])。全因死亡率(ACM)的 HR 为 0.52(95% CI 0.38-0.72),MI/卒中/ACM 复合结局的 HR 为 0.83(95% CI 0.70-0.98)。恩格列净与 LLA 和骨折风险相似,DKA 风险增加(HR 1.71 [95% CI 1.08-2.71]),AKI 风险降低(HR 0.60 [95% CI 0.43-0.85])。
在临床实践中,起始使用恩格列净而非 DPP-4 抑制剂与 HHF、ACM 和 MI/卒中/ACM 风险降低、MI/卒中风险相似以及与已发表资料一致的安全性特征相关。