Unit of Infectious Diseases, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden.
Department of Infectious Diseases, Karolinska University Hospital, Stockholm, Sweden.
Eur J Clin Microbiol Infect Dis. 2021 Mar;40(3):525-534. doi: 10.1007/s10096-020-04035-y. Epub 2020 Sep 18.
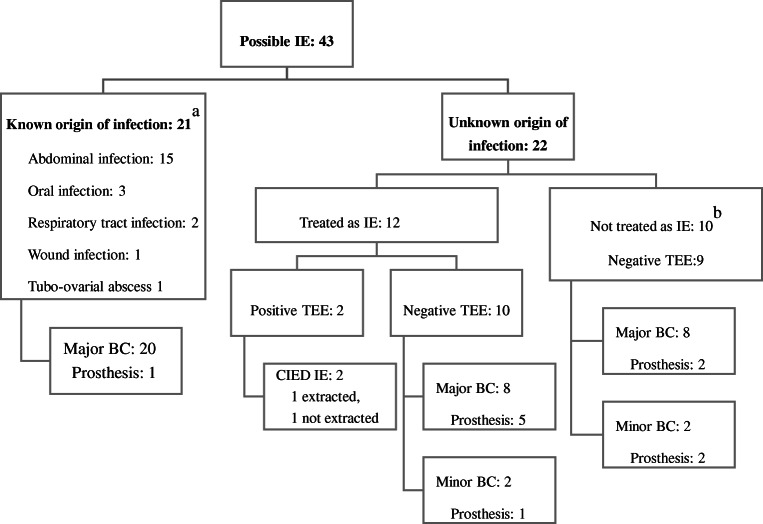
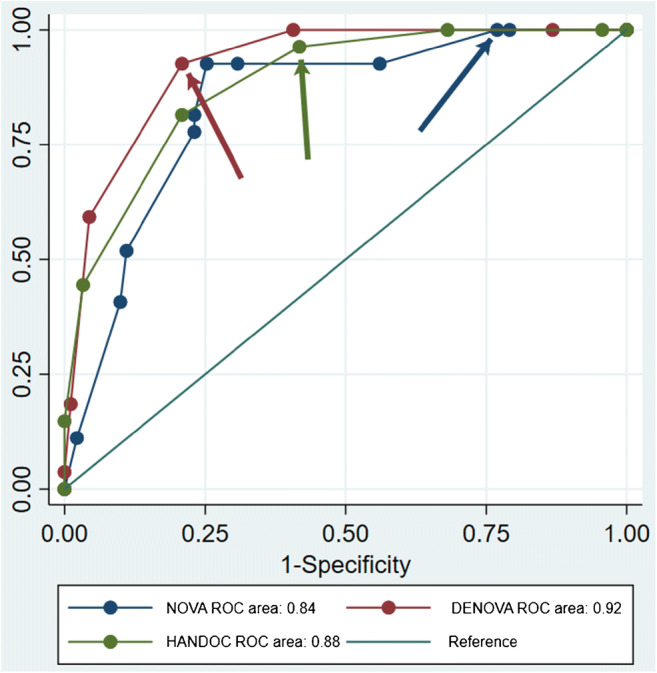
The objective was to describe the epidemiology, bacteriology, clinical presentation, risk factors for endocarditis (IE), diagnostic workup, and outcome of patients with bacteremia caused by the non-influenzae Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella genera (HACEK). A retrospective population-based cohort of patients with bacteremia collected from 2012 to 2017 was identified. Clinical data from identified patients were collected from medical records to classify patients, calculate incidences, analyze risk factors of IE, and describe the management and outcome of the cohort. A total of 118 episodes of HACEK bacteremia were identified, of which 27 were definite IE. The incidence of HACEK bacteremia was 5.2 and of HACEK IE 1.2 episodes per 1,000,000 inhabitants per year. Other focal infections were identified in 55 of 118 of the episodes, most commonly within the abdomen (26 episodes). The propensity to cause IE ranged from 62 in Aggregatibacter actinomycetemcomitans to 6% in Eikenella. Risk factors for IE were cardiac implantable electronical device, predisposing cardiac conditions, community acquisition, long duration of symptoms, multiple positive blood cultures, fever, heart murmur, embolization, and unknown origin of infection. The scoring system DENOVA developed to predict IE in bacteremia with Enterococcus faecalis also had a high sensitivity and specificity for predicting IE in HACEK bacteremia. The 30-day mortality was 4% in IE and 15% in non-IE bacteremia, and only one case of relapse was found. IE is common in bacteremia with Aggregatibacter, Cardiobacterium, and Kingella but relatively rare in Haemophilus and Eikenella. Treatment failures are very rare, and DENOVA can be used to evaluate the need for transesophageal echocardiography.
目的在于描述由非流感嗜血杆菌、聚集性放线杆菌、心杆菌、爱肯菌和金氏杆菌属(HACEK)引起的菌血症患者的流行病学、细菌学、临床表现、心内膜炎(IE)的危险因素、诊断方法和结局。从 2012 年至 2017 年,我们确定了一项基于人群的菌血症患者回顾性队列研究。从病历中收集了确定的患者的临床数据,以对患者进行分类、计算发病率、分析 IE 的危险因素,并描述队列的管理和结局。共确定了 118 例 HACEK 菌血症,其中 27 例为明确的 IE。HACEK 菌血症的发病率为每年每 100 万人 5.2 例,HACEK IE 为 1.2 例。118 例中,55 例有其他局部感染,最常见的是腹部(26 例)。引起 IE 的倾向范围从 62%的聚集性放线杆菌到 6%的爱肯菌。IE 的危险因素包括心脏植入电子设备、潜在的心脏疾病、社区获得性感染、症状持续时间长、多次血培养阳性、发热、心脏杂音、栓塞和感染源不明。为预测粪肠球菌引起的菌血症中的 IE 而开发的 DENOVA 评分系统,对于预测 HACEK 菌血症中的 IE 也具有较高的敏感性和特异性。IE 的 30 天死亡率为 4%,非 IE 菌血症为 15%,仅发现 1 例复发。IE 在Aggregatibacter、Cardiobacterium 和 Kingella 引起的菌血症中很常见,但在 Haemophilus 和 Eikenella 引起的菌血症中相对少见。治疗失败非常罕见,DENOVA 可用于评估是否需要行经食管超声心动图检查。