Department of Surgery, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
Department of Family Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
PLoS One. 2020 Sep 18;15(9):e0239082. doi: 10.1371/journal.pone.0239082. eCollection 2020.
The majority of clinical decision rules for prediction of intracranial injury in patients with mild traumatic brain injury (TBI) were developed from high-income countries. The application of these rules in low or middle-income countries, where the primary mechanism of injury was traffic accidents, is questionable.
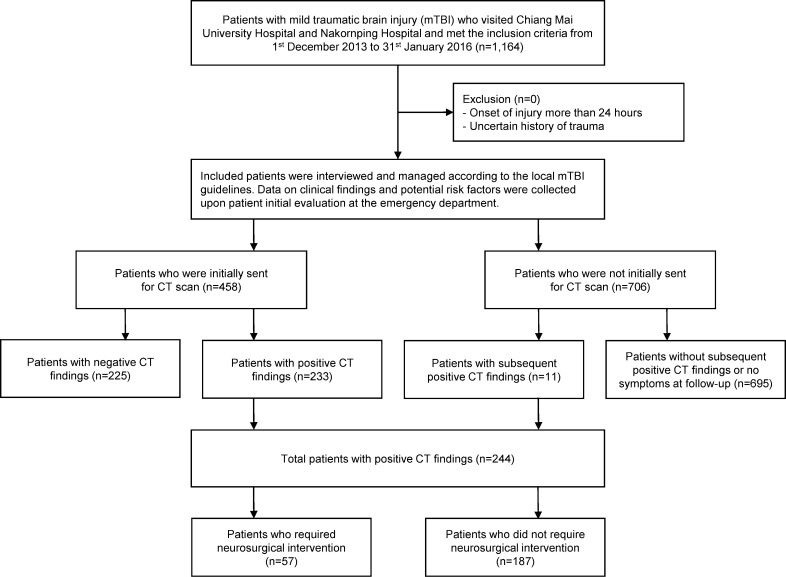
We developed two practical decision rules from a secondary analysis of a multicenter, prospective cohort of 1,164 patients with mild TBI who visited the emergency departments from 2013 to 2016. The clinical endpoints were the presence of any intracranial injury on CT scans and the requirement of neurosurgical interventions within seven days of onset.
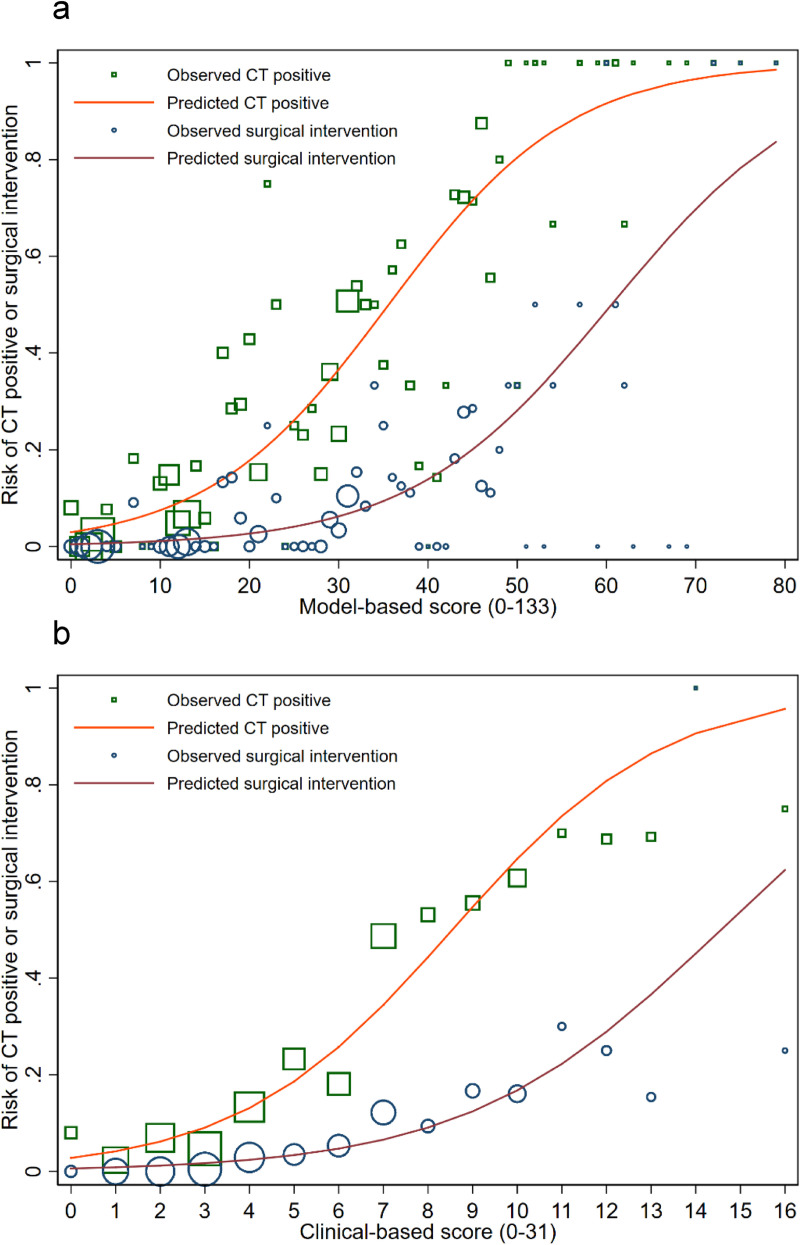
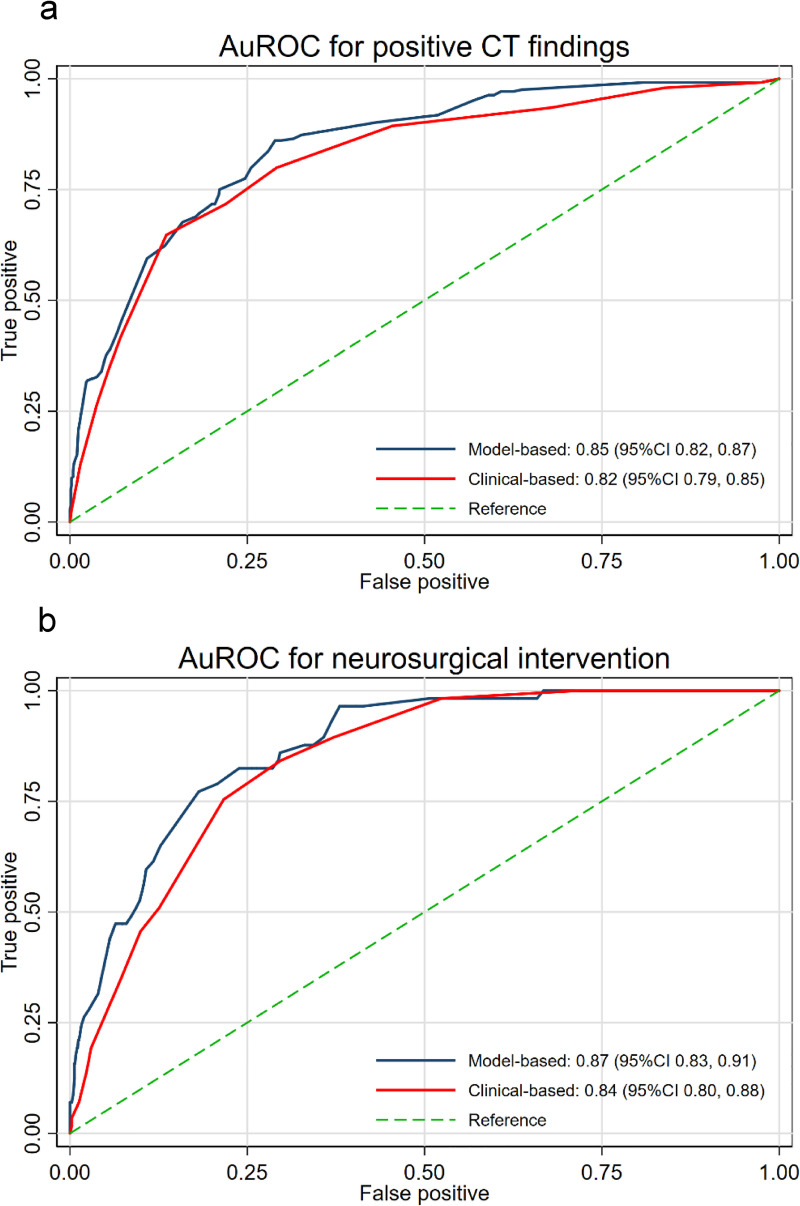
Thirteen predictors were included in both models, which were age ≥60 years, dangerous mechanism of injury, diffuse headache, vomiting >2 episodes, loss of consciousness, posttraumatic amnesia, posttraumatic seizure, history of anticoagulant use, presence of neurological deficits, significant wound at the scalp, signs of skull base fracture, palpable stepping at the skull, and GCS <15 at 2 hours. For the model-based score, the area under the receiver operating characteristic curve (AuROC) was 0.85 (95%CI 0.82, 0.87) for positive CT results and 0.87 (95%CI 0.83, 0.91) for requirement of neurosurgical intervention. For the clinical-based score, the AuROC for positive CT results and requirement of neurosurgical intervention was 0.82 (95%CI 0.79, 0.85) and 0.84 (95%CI 0.80, 0.88), respectively.
The models delivered good calibration and excellent discrimination both in the development and internal validation cohort. These rules can be used as assisting tools in risk stratification of patients with mild TBI to be sent for CT scans or admitted for clinical observation.
大多数用于预测轻度创伤性脑损伤(TBI)患者颅内损伤的临床决策规则都是在高收入国家开发的。这些规则在主要损伤机制为交通事故的低收入和中等收入国家的应用是值得怀疑的。
我们从 2013 年至 2016 年期间在多家急诊中心就诊的 1164 例轻度 TBI 患者的多中心前瞻性队列的二次分析中开发了两个实用的决策规则。临床终点是 CT 扫描上存在任何颅内损伤和发病后 7 天内需要神经外科干预。
两个模型均纳入了 13 个预测因素,分别是年龄≥60 岁、危险的损伤机制、弥漫性头痛、呕吐≥2 次、意识丧失、创伤后遗忘、创伤后癫痫发作、抗凝药物使用史、神经功能缺损、头皮有明显伤口、颅底骨折迹象、可触及颅骨台阶、GCS 在 2 小时时<15。对于基于模型的评分,ROC 曲线下面积(AuROC)为阳性 CT 结果为 0.85(95%CI 0.82,0.87),需要神经外科干预为 0.87(95%CI 0.83,0.91)。对于基于临床的评分,阳性 CT 结果和需要神经外科干预的 AuROC 分别为 0.82(95%CI 0.79,0.85)和 0.84(95%CI 0.80,0.88)。
这些模型在开发和内部验证队列中均具有良好的校准和出色的区分能力。这些规则可作为轻度 TBI 患者进行 CT 扫描或接受临床观察的风险分层辅助工具。