Sheriff Faheem, Castro Pedro, Kozberg Mariel, LaRose Sarah, Monk Andrew, Azevedo Elsa, Li Karen, Jafari Sameen, Rao Shyam, Otite Fadar Oliver, Khawaja Ayaz, Sorond Farzaneh, Feske Steven, Tan Can Ozan, Vaitkevicius Henrikas
Department of Neurology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA.
Department of Neurocritical Care, Brigham and Women's Hospital, 75 Francis Street, Boston, MA 02115, USA.
Brain Sci. 2020 Sep 16;10(9):641. doi: 10.3390/brainsci10090641.
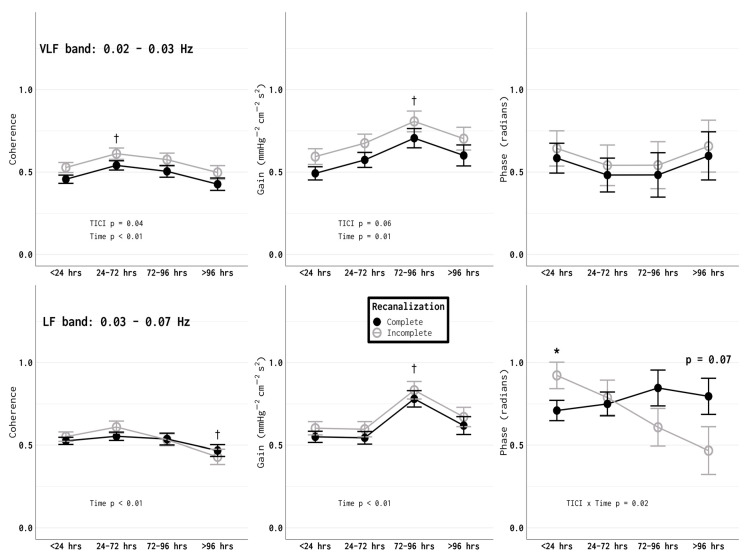
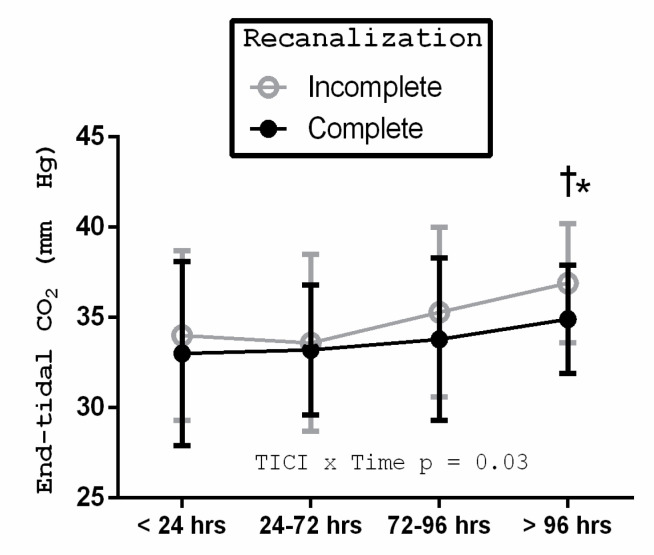
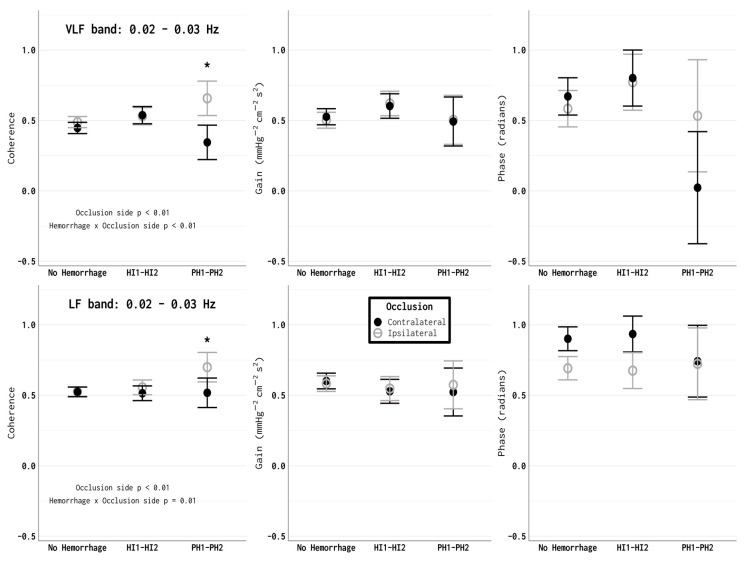
The development of the endovascular thrombectomy (EVT) technique has revolutionized acute stroke management for patients with large vessel occlusions (LVOs). The impact of successful recanalization using an EVT on autoregulatory profiles is unknown. A more complete understanding of cerebral autoregulation in the context of EVT may assist with post-procedure hemodynamic optimization to prevent complications. We examined cerebral autoregulation in 107 patients with an LVO in the anterior circulation (proximal middle cerebral artery (M1/2) and internal cerebral artery (ICA) terminus) who had been treated using an EVT. Dynamic cerebral autoregulation was assessed at multiple time points, ranging from less than 24 hours to 5 days following last seen well (LSW) time, using transcranial Doppler ultrasound recordings and transfer function analysis. Complete (Thrombolysis in Cerebral Infarction (TICI) 3) recanalization was associated with a more favorable autoregulation profile compared with TICI 2b or poorer recanalization ( < 0.05), which is an effect that was present after accounting for differences in the infarct volumes. Less effective autoregulation in the first 24 h following the LSW time was associated with increased rates of parenchymal hematoma types 1 and 2 hemorrhagic transformations (PH1-PH2). These data suggest that patients with incomplete recanalization and poor autoregulation (especially within the first 24 h post-LSW time) may warrant closer blood pressure monitoring and control in the first few days post ictus.
血管内血栓切除术(EVT)技术的发展彻底改变了大血管闭塞(LVO)患者的急性卒中治疗。使用EVT成功再通对自动调节曲线的影响尚不清楚。在EVT背景下更全面地了解脑自动调节可能有助于术后血流动力学优化以预防并发症。我们研究了107例前循环LVO(大脑中动脉近端(M1/2)和大脑内动脉(ICA)末端)且接受了EVT治疗的患者的脑自动调节情况。使用经颅多普勒超声记录和传递函数分析,在最后看起来正常(LSW)时间后的多个时间点(从不到24小时到5天)评估动态脑自动调节。与TICI 2b或再通较差相比,完全(脑梗死溶栓(TICI)3级)再通与更有利的自动调节曲线相关(<0.05),在考虑梗死体积差异后该效应仍然存在。在LSW时间后的最初24小时内自动调节效果较差与1型和2型实质血肿出血转化(PH1-PH2)的发生率增加相关。这些数据表明,再通不完全且自动调节较差的患者(尤其是在LSW时间后的最初24小时内)可能需要在发病后的头几天进行更密切的血压监测和控制。