Radcliffe Department of Medicine, Level 4 Academic Block, University of Oxford, John Radcliffe Hospital, Headley Way, Oxford, OX3 9DU, UK.
Adult Intensive Care Unit, John Radcliffe Hospital, Oxford University Hospitals NHS Foundation Trust, Oxford, UK.
Crit Care. 2020 Sep 18;24(1):561. doi: 10.1186/s13054-020-03260-3.
Optimal prophylactic and therapeutic management of thromboembolic disease in patients with COVID-19 remains a major challenge for clinicians. The aim of this study was to define the incidence of thrombotic and haemorrhagic complications in critically ill patients with COVID-19. In addition, we sought to characterise coagulation profiles using thromboelastography and explore possible biological differences between patients with and without thrombotic complications.
We conducted a multicentre retrospective observational study evaluating all the COVID-19 patients received in four intensive care units (ICUs) of four tertiary hospitals in the UK between March 15, 2020, and May 05, 2020. Clinical characteristics, laboratory data, thromboelastography profiles and clinical outcome data were evaluated between patients with and without thrombotic complications.
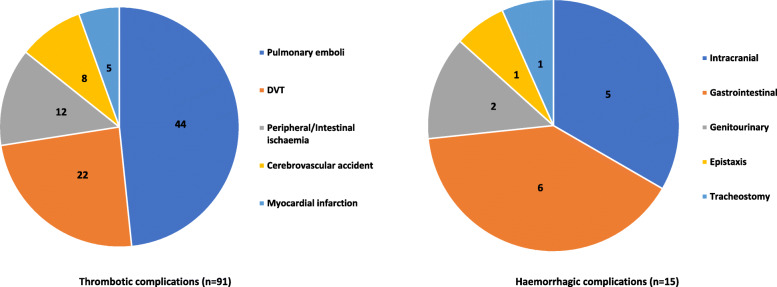
A total of 187 patients were included. Their median (interquartile (IQR)) age was 57 (49-64) years and 124 (66.3%) patients were male. Eighty-one (43.3%) patients experienced one or more clinically relevant thrombotic complications, which were mainly pulmonary emboli (n = 42 (22.5%)). Arterial embolic complications were reported in 25 (13.3%) patients. ICU length of stay was longer in patients with thrombotic complications when compared with those without. Fifteen (8.0%) patients experienced haemorrhagic complications, of which nine (4.8%) were classified as major bleeding. Thromboelastography demonstrated a hypercoagulable profile in patients tested but lacked discriminatory value between those with and without thrombotic complications. Patients who experienced thrombotic complications had higher D-dimer, ferritin, troponin and white cell count levels at ICU admission compared with those that did not.
Critically ill patients with COVID-19 experience high rates of venous and arterial thrombotic complications. The rates of bleeding may be higher than previously reported and re-iterate the need for randomised trials to better understand the risk-benefit ratio of different anticoagulation strategies.
在 COVID-19 患者中,优化血栓栓塞性疾病的预防和治疗管理仍然是临床医生面临的主要挑战。本研究旨在确定危重症 COVID-19 患者中血栓和出血并发症的发生率。此外,我们还试图使用血栓弹力描记术描述凝血谱,并探索有血栓并发症和无血栓并发症患者之间可能存在的生物学差异。
我们进行了一项多中心回顾性观察性研究,评估了 2020 年 3 月 15 日至 2020 年 5 月 5 日期间英国四家三级医院的四个重症监护病房(ICU)收治的所有 COVID-19 患者。评估了有和无血栓并发症患者的临床特征、实验室数据、血栓弹力描记术谱和临床结局数据。
共纳入 187 例患者。他们的中位(四分位间距(IQR))年龄为 57(49-64)岁,124 例(66.3%)为男性。81 例(43.3%)患者经历了一次或多次有临床意义的血栓并发症,主要为肺栓塞(n=42(22.5%))。动脉栓塞并发症发生于 25 例(13.3%)患者中。与无血栓并发症的患者相比,有血栓并发症的患者 ICU 住院时间更长。15 例(8.0%)患者发生出血并发症,其中 9 例(4.8%)为大出血。进行血栓弹力描记术检查的患者表现出高凝状态,但缺乏对有和无血栓并发症患者的鉴别价值。与无血栓并发症的患者相比,有血栓并发症的患者在入住 ICU 时的 D-二聚体、铁蛋白、肌钙蛋白和白细胞计数水平更高。
COVID-19 危重症患者发生静脉和动脉血栓并发症的比例较高。出血的发生率可能高于之前的报道,这再次强调需要进行随机试验以更好地了解不同抗凝策略的风险效益比。