Koike Haruki, Katsuno Masahisa
Department of Neurology, Nagoya University Graduate School of Medicine, Nagoya, Japan.
Neurol Ther. 2020 Dec;9(2):317-333. doi: 10.1007/s40120-020-00210-7. Epub 2020 Sep 18.
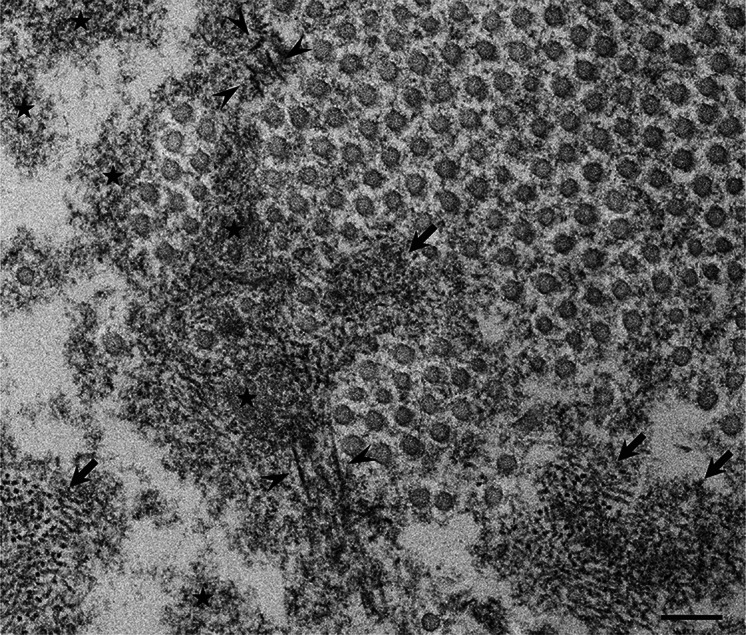
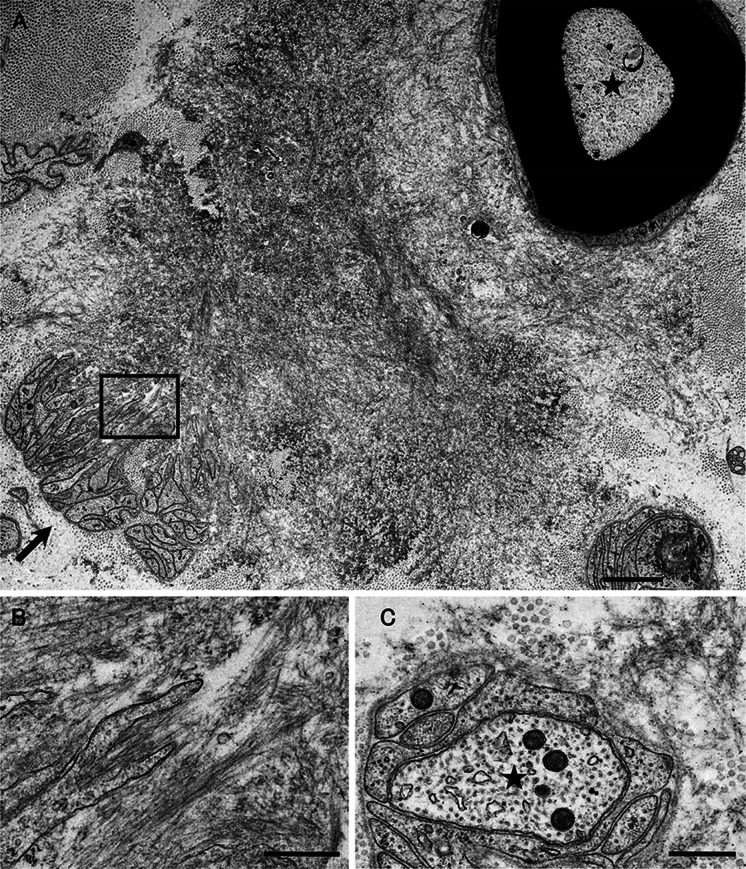
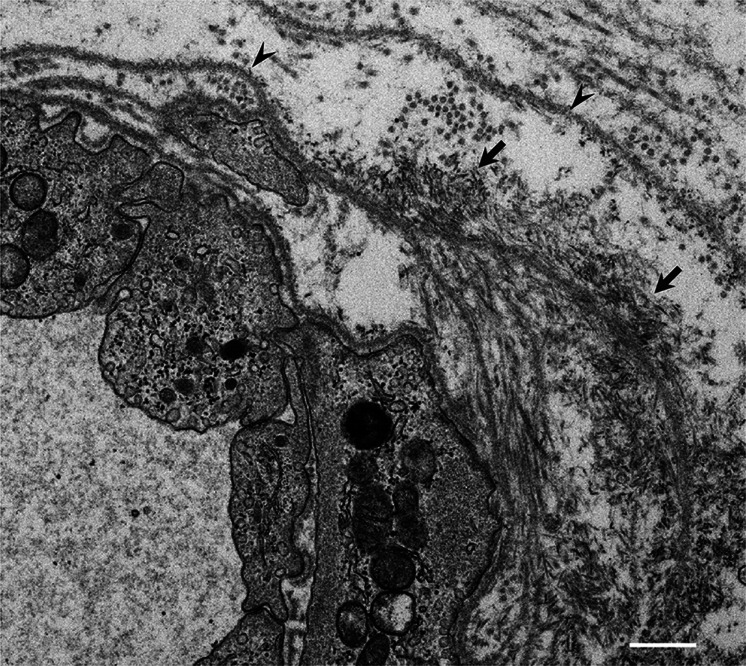
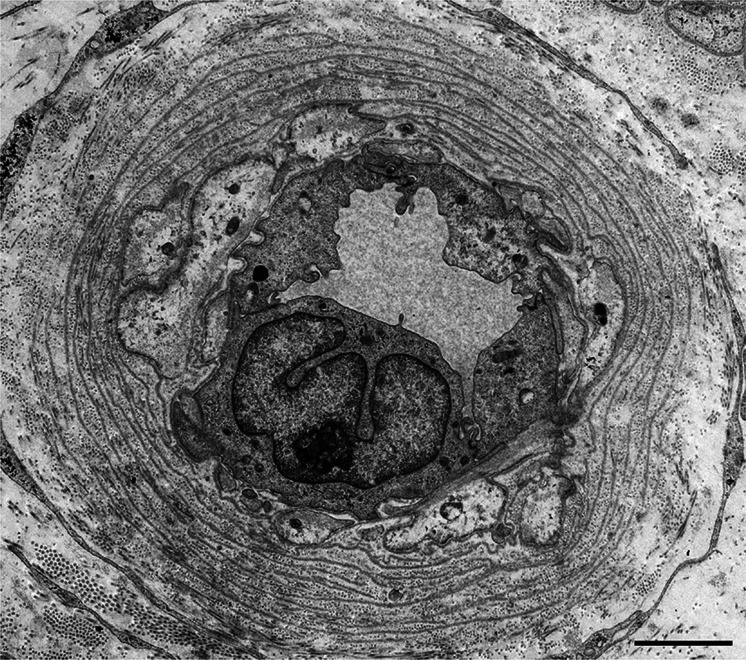
ATTR amyloidosis is caused by systemic deposition of transthyretin (TTR) and comprises ATTRwt (wt for wild-type) amyloidosis, ATTRv (v for variant) amyloidosis, and acquired ATTR amyloidosis after domino liver transplantation. ATTRwt amyloidosis has classically been regarded as cardiomyopathy found in the elderly, whereas carpal tunnel syndrome has also become a major initial manifestation. The phenotypes of ATTRv amyloidosis are diverse and include neuropathy, cardiomyopathy, and oculoleptomeningeal involvement as the predominant features, depending on the mutation and age of onset. In addition to variant TTR, the deposition of wild-type TTR plays a significant role, even in patients with ATTRv amyloidosis. The formation of amyloid fibrils tends to occur in association with the basement membrane. The thickening or reduplication of the basement membrane surrounding endoneurial microvessels, which is similar to diabetic neuropathy, is observed in ATTRv amyloidosis, suggesting that common mechanisms, such as an accumulation of advanced glycation end products, may participate in the disease process. In addition to direct damage caused by amyloid fibrils, recent studies have suggested that the toxicity of nonfibrillar TTRs, such as TTR oligomers, participates in the process of tissue damage. Although liver transplantation has been performed for patients with ATTRv amyloidosis since 1990, late-onset patients were not eligible for this treatment. However, as the efficacy of orally administered tafamidis and diflunisal, which stabilize TTR tetramers, was suggested in the early 2010s, such late-onset patients have also become targets for disease-modifying therapies. Additionally, recent studies of small interfering RNA (patisiran) and antisense oligonucleotide (inotersen) therapies have demonstrated the efficacy of these gene-silencing agents. A strategy for monitoring patients that enables the choice of an appropriate treatment from comprehensive and long-term viewpoints should be established. As many patients with ATTR amyloidosis are aged and have heart failure, they are at increased risk of aggravation if they are infected by SARS-CoV2. The optimal interval of evaluation should also be considered, particularly in this COVID-19 era.
转甲状腺素蛋白(TTR)的系统性沉积会引发转甲状腺素蛋白淀粉样变性(ATTR),它包括野生型转甲状腺素蛋白淀粉样变性(ATTRwt,wt代表野生型)、变异型转甲状腺素蛋白淀粉样变性(ATTRv,v代表变异型)以及多米诺肝移植后获得性ATTR淀粉样变性。ATTRwt淀粉样变性传统上被认为是老年人中出现的心肌病,而腕管综合征也已成为主要的初始表现。ATTRv淀粉样变性的表型多样,根据突变情况和发病年龄,主要特征包括神经病变、心肌病以及眼软脑膜受累。除了变异型TTR,野生型TTR的沉积也起着重要作用,即使在ATTRv淀粉样变性患者中也是如此。淀粉样纤维的形成往往与基底膜相关。在ATTRv淀粉样变性中观察到,神经内膜微血管周围基底膜增厚或重复,这与糖尿病性神经病变相似,提示晚期糖基化终产物的积累等共同机制可能参与疾病过程。除了淀粉样纤维造成的直接损伤,最近的研究表明,非纤维状TTR(如TTR寡聚体)的毒性也参与组织损伤过程。自1990年以来,肝移植已用于ATTRv淀粉样变性患者,但晚发型患者不符合这种治疗条件。然而,随着21世纪10年代初口服的稳定TTR四聚体的他氟米特和双氟尼酸的疗效得到证实,这类晚发型患者也成为疾病修饰疗法的目标。此外,最近对小干扰RNA(帕替拉韦)和反义寡核苷酸(依诺特森)疗法的研究证明了这些基因沉默剂的疗效。应该建立一种患者监测策略,以便能够从全面和长期的角度选择合适的治疗方法。由于许多ATTR淀粉样变性患者年事已高且患有心力衰竭,如果感染严重急性呼吸综合征冠状病毒2(SARS-CoV2),他们病情加重的风险会增加。尤其在这个新冠病毒病(COVID-19)时代,还应考虑最佳评估间隔。