Klinik und Poliklinik für Kardiologie, Universitätsklinikum Leipzig, Liebigstraße 20, 04103, Leipzig, Germany.
AMGEN Europe GmbH, Rotkreuz, Switzerland.
Clin Res Cardiol. 2022 Mar;111(3):243-252. doi: 10.1007/s00392-020-01740-8. Epub 2020 Sep 19.
Many patients at very-high atherosclerotic cardiovascular disease risk do not reach guideline-recommended targets for LDL-C. There is a lack of data on real-world use of non-statin lipid-lowering therapies (LLT) and little is known on the effectiveness of fixed-dose combinations (FDC). We therefore studied prescription trends in oral non-statin LLT and their effects on LDL-C.
A retrospective analysis was conducted of electronic medical records of outpatients at very-high cardiovascular risk treated by general practitioners (GPs) and cardiologists, and prescribed LLT in Germany between 2013 and 2018.
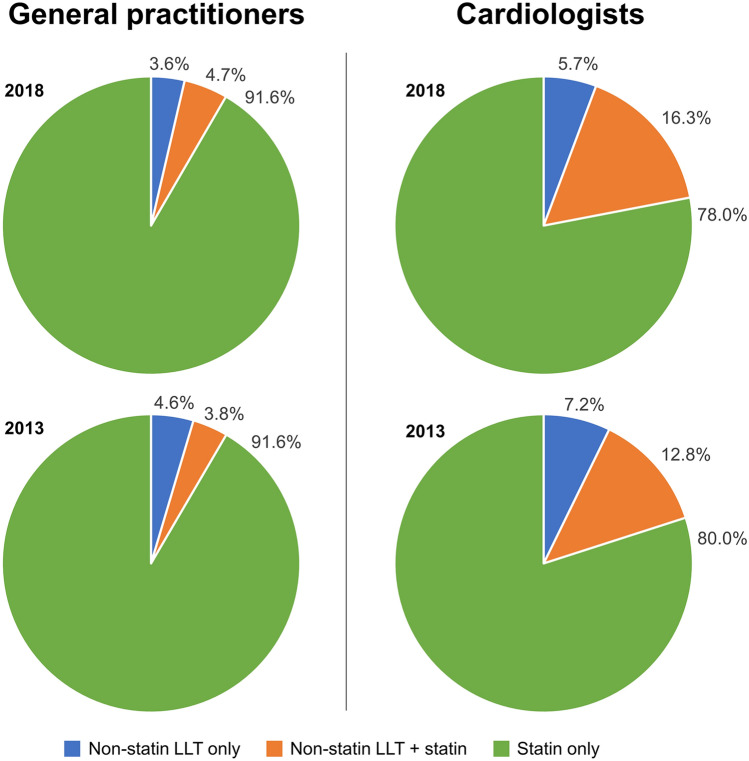
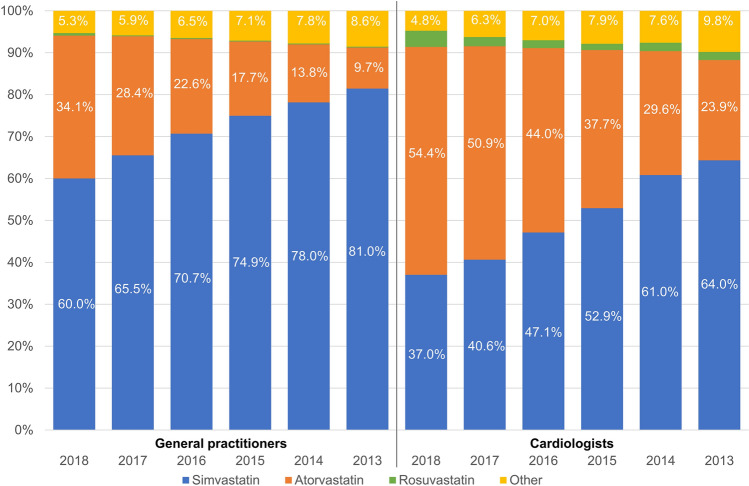
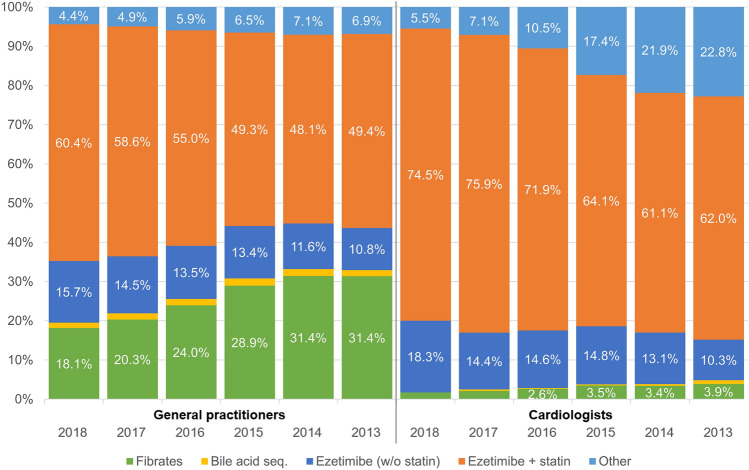
Data from 311,242 patients were analysed. Prescriptions for high-potency statins (atorvastatin and rosuvastatin) increased from 10.4% and 25.8% of patients treated by GPs and cardiologists, respectively, in 2013, to 34.7% and 58.3% in 2018. Prescription for non-statin LLT remained stable throughout the period and low especially for GPs. Ezetimibe was the most prescribed non-statin LLT in 2018 (GPs, 76.1%; cardiologists, 92.8%). Addition of ezetimibe in patients already prescribed a statin reduced LDL-C by an additional 23.8% (32.3 ± 38.4 mg/dL), with a greater reduction with FDC [reduction 28.4% (40.0 ± 39.1 mg/dL)] as compared to separate pills [19.4% (27.5 ± 33.8 mg/dL)]; p < 0.0001. However, only a small proportion of patients reached the recommended LDL-C level of < 70 mg/dL (31.5% with FDC and 21.0% with separate pills).
Prescription for high-potency statins increased over time. Non-statin LLT were infrequently prescribed by GPs. The reduction in LDL-C when statin and ezetimibe were prescribed in combination was considerably larger for FDC; however, a large proportion of patients still remained with uncontrolled LDL-C levels.
许多极高心血管疾病风险的患者未达到 LDL-C 的指南推荐目标。关于现实世界中使用非他汀类降脂疗法(LLT)的数据很少,对固定剂量复方制剂(FDC)的疗效知之甚少。因此,我们研究了口服非他汀类 LLT 的处方趋势及其对 LDL-C 的影响。
对德国全科医生和心脏病专家治疗的极高心血管风险的门诊患者的电子病历进行回顾性分析,这些患者在 2013 年至 2018 年间接受了 LLT 治疗。
对 311242 名患者的数据进行了分析。高剂量他汀类药物(阿托伐他汀和瑞舒伐他汀)的处方在全科医生和心脏病专家治疗的患者中分别从 2013 年的 10.4%和 25.8%增加到 2018 年的 34.7%和 58.3%。在此期间,非他汀类 LLT 的处方一直保持稳定,尤其是对全科医生来说更是如此。依折麦布是 2018 年最常开的非他汀类 LLT(全科医生,76.1%;心脏病专家,92.8%)。在已服用他汀类药物的患者中加用依折麦布可使 LDL-C 进一步降低 23.8%(32.3±38.4mg/dL),与单独服用药物相比(降低 19.4%(27.5±33.8mg/dL)),FDC 降低的幅度更大[降低 28.4%(40.0±39.1mg/dL)];p<0.0001。然而,只有一小部分患者达到了推荐的 LDL-C 水平<70mg/dL(FDC 为 31.5%,单独服用为 21.0%)。
高剂量他汀类药物的处方随着时间的推移而增加。全科医生很少开非他汀类 LLT。当他汀类药物和依折麦布联合使用时,FDC 降低 LDL-C 的效果要大得多;然而,仍有很大一部分患者 LDL-C 水平未得到控制。