Daniels S L, Lee M J, George J, Kerr K, Moug S, Wilson T R, Brown S R, Wyld L
Academic Directorate of General Surgery, Sheffield, UK.
Department of Oncology and Metabolism, University of Sheffield, Sheffield, UK.
BJS Open. 2020 Sep 22;4(6):1022-41. doi: 10.1002/bjs5.50347.
Prehabilitation has emerged as a strategy to prepare patients for elective abdominal cancer surgery with documented improvements in postoperative outcomes. The aim of this study was to assess the evidence for prehabilitation interventions of relevance to the older adult.
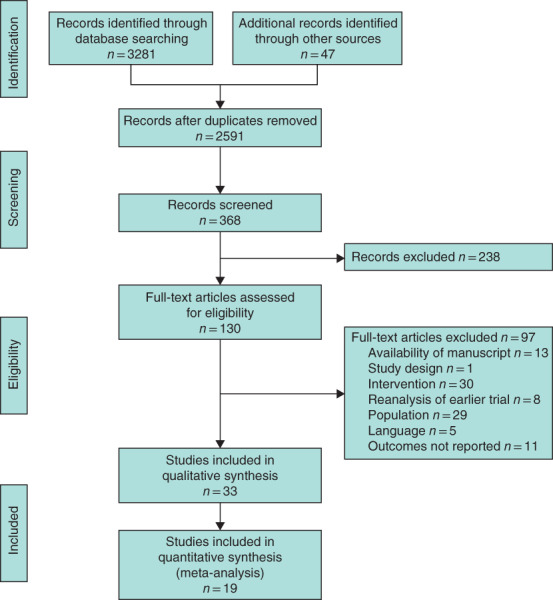
Systematic searches were conducted using MEDLINE, Web of Science, Scopus, CINAHL and PsychINFO. Studies of preoperative intervention (prehabilitation) in patients undergoing abdominal cancer surgery reporting postoperative outcomes were included. Age limits were not set as preliminary searches revealed this would be too restrictive. Articles were screened and selected based on PRISMA guidelines, and assessment of bias was performed. Qualitative, quantitative and meta-analyses of data were conducted as appropriate.
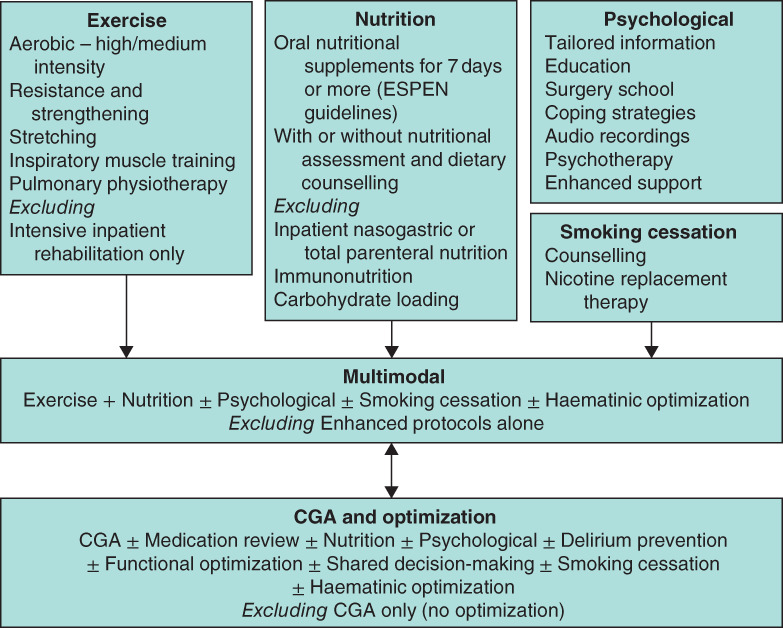
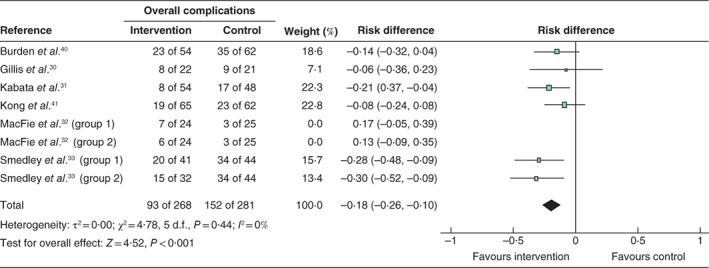
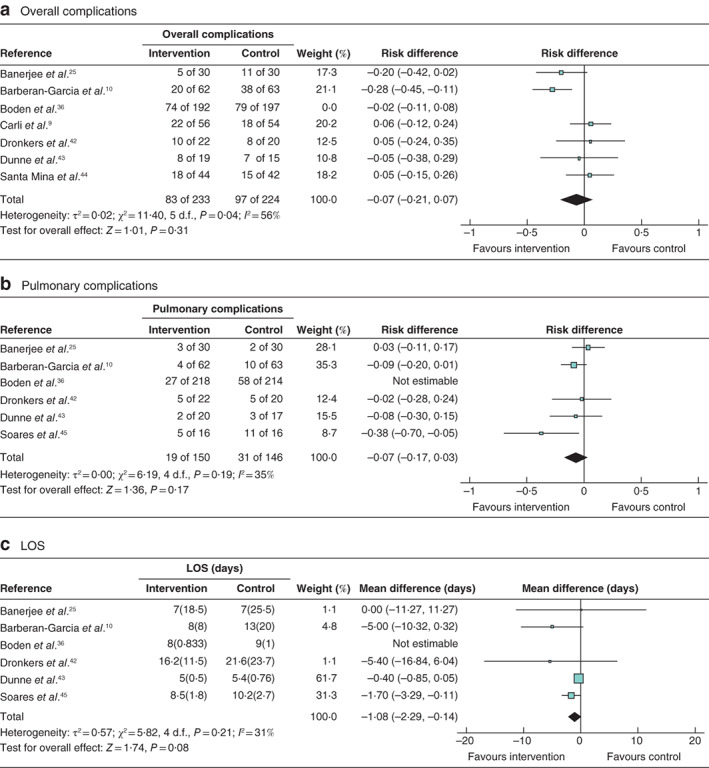
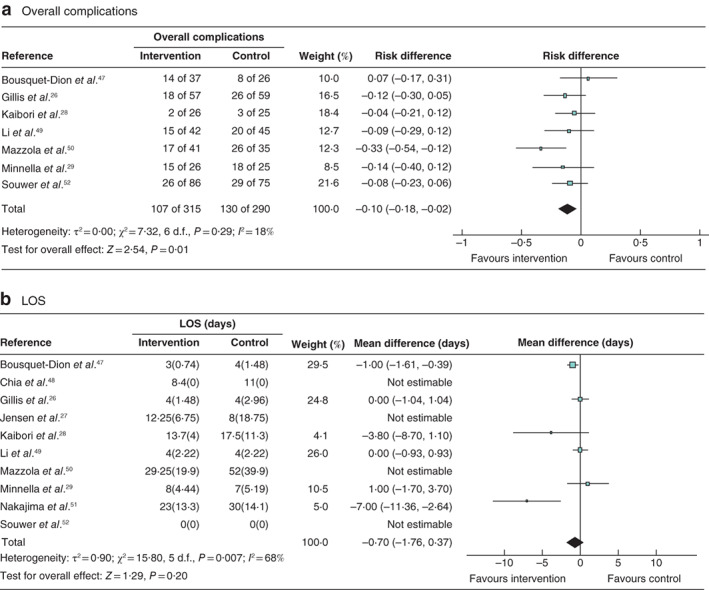
Thirty-three studies (3962 patients) were included. Interventions included exercise, nutrition, psychological input, comprehensive geriatric assessment and optimization, smoking cessation and multimodal (two or more interventions). Nine studies purposely selected high-risk, frail or older patients. Thirty studies were at moderate or high risk of bias. Ten studies individually reported benefits in complication rates, with meta-analyses for overall complications demonstrating significant benefit: multimodal (risk difference -0·1 (95 per cent c.i. -0·18 to -0·02); P = 0·01, I = 18 per cent) and nutrition (risk difference -0·18 (-0·26 to -0·10); P < 0·001, I = 0 per cent). Seven studies reported reductions in length of hospital stay, with no differences on meta-analysis.
The conclusions of this review are limited by the quality of the included studies, and the heterogeneity of interventions and outcome measures reported. Exercise, nutritional and multimodal prehabilitation may reduce morbidity after abdominal surgery, but data specific to older patients are sparse.
术前康复已成为一种为择期腹部癌症手术患者做准备的策略,术后结果有明显改善。本研究的目的是评估与老年患者相关的术前康复干预措施的证据。
使用MEDLINE、科学网、Scopus、护理学与健康领域数据库(CINAHL)和心理学文摘数据库(PsychINFO)进行系统检索。纳入报告腹部癌症手术患者术后结果的术前干预(术前康复)研究。未设定年龄限制,因为初步检索显示这样限制过严。根据系统评价和Meta分析的首选报告项目(PRISMA)指南筛选和选择文章,并进行偏倚评估。酌情对数据进行定性、定量和Meta分析。
纳入33项研究(3962例患者)。干预措施包括运动、营养、心理干预、综合老年评估与优化、戒烟和多模式干预(两种或更多干预措施)。9项研究特意选择了高危、体弱或老年患者。30项研究存在中度或高度偏倚风险。10项研究分别报告了并发症发生率方面的益处,总体并发症的Meta分析显示有显著益处:多模式干预(风险差 -0.1(95%置信区间 -0.18至 -0.02);P = 0.01,I² = 18%)和营养干预(风险差 -0.18(-0.26至 -0.10);P < 0.001,I² = 0%)。7项研究报告住院时间缩短,Meta分析无差异。
本综述的结论受到纳入研究质量以及所报告的干预措施和结果测量方法异质性的限制。运动、营养和多模式术前康复可能降低腹部手术后的发病率,但针对老年患者的具体数据较少。