Département d'Ophtalmologie, CHU Charles Nicolle, F-76000, Rouen, France.
Centre de référence des dermatoses bulleuses toxiques et toxidermies graves TOXIBUL, Créteil, France.
Orphanet J Rare Dis. 2020 Sep 22;15(1):259. doi: 10.1186/s13023-020-01538-x.
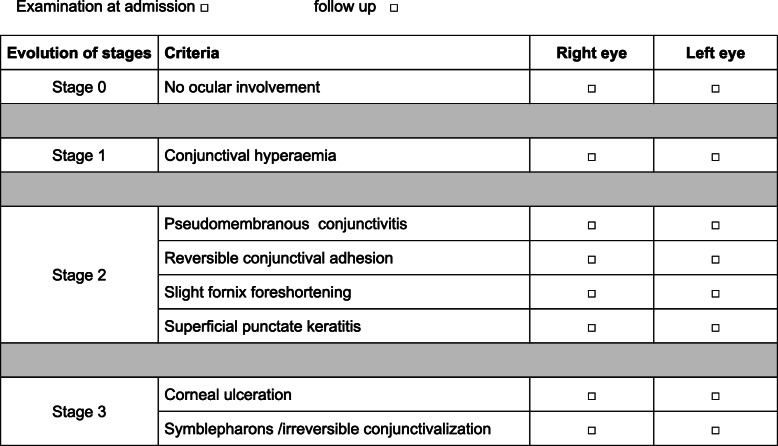
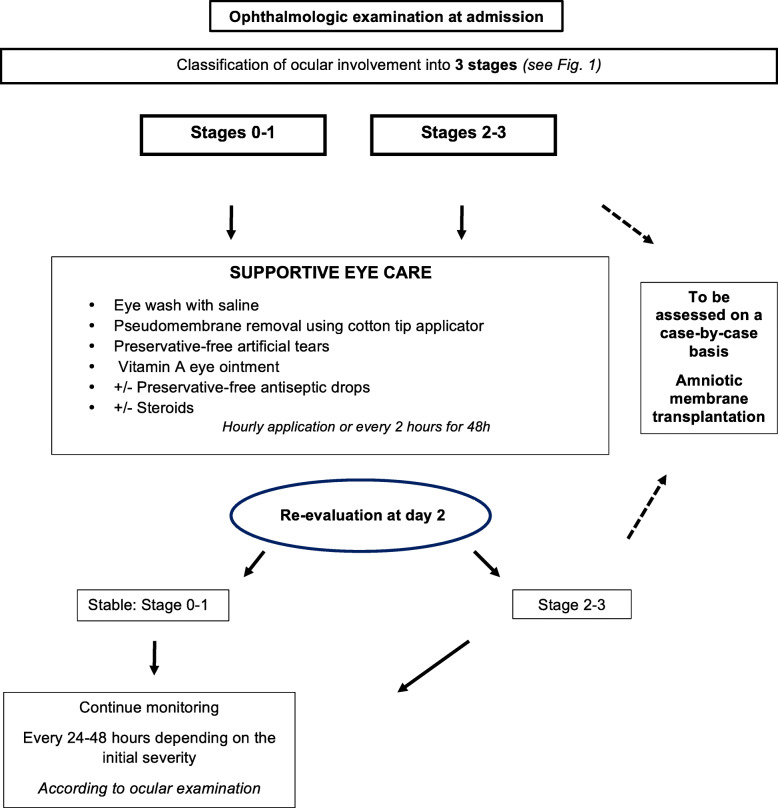
Stevens-Johnson Syndrome (SJS) and toxic epidermal necrolysis (TEN) can lead to severe ophthalmologic sequelae. The main risk factor is the severity of the initial ocular involvement. There are no recommendations for ocular management during acute phase.We conducted a national audit of current practice in the 11 sites of the French reference center for toxic bullous dermatoses and a review of the literature to establish therapeutic consensus guidelines. We sent a questionnaire on ocular management practices in SJS/ TEN during acute phase to ophthalmologists and dermatologists. The survey focused on ophthalmologist opinion, pseudomembrane removal, topical ocular treatment (i.e. corticosteroids, antibiotics, antiseptics, artificial tear eye drops, vitamin A ointment application), amniotic membrane transplantation, symblepharon ring use, and systemic corticosteroid therapy for ophthalmologic indication. Nine of 11 centers responded. All requested prompt ophthalmologist consultation. The majority performed pseudomembrane removal, used artificial tears, and vitamin A ointment (8/9, 90%). Combined antibiotic-corticosteroid or corticosteroid eye drops were used in 6 centers (67%), antibiotics alone and antiseptics in 3 centers (33%). Symblepharon ring was used in 5 centers (55%) if necessary. Amniotic membrane transplantation was never performed systematically and only according to the clinical course. Systemic corticosteroid therapy was occasionally used (3/9, 33%) and discussed on a case-by-case basis.The literature about ocular management practice in SJS/ TEN during acute phase is relatively poor. The role of specific treatments such as local or systemic corticosteroid therapy is not consensual. The use of preservatives, often present in eye drops and deleterious to the ocular surface, is to be restricted. Early amniotic membrane transplantation seems to be promising.
史蒂文斯-约翰逊综合征(SJS)和中毒性表皮坏死松解症(TEN)可导致严重的眼部后遗症。主要的风险因素是初始眼部受累的严重程度。目前没有关于急性阶段眼部管理的建议。我们对法国毒性大疱性皮肤病参考中心的 11 个地点的当前实践进行了全国性审计,并对文献进行了回顾,以制定治疗共识指南。我们向眼科医生和皮肤科医生发送了一份关于 SJS/TEN 急性阶段眼部管理实践的问卷。调查重点是眼科医生的意见、假膜去除、局部眼部治疗(即皮质类固醇、抗生素、防腐剂、人工泪液滴眼剂、维生素 A 软膏应用)、羊膜移植、睑球粘连环使用以及出于眼科适应证的全身皮质类固醇治疗。11 个中心中有 9 个做出了回应。所有中心都要求尽快进行眼科会诊。大多数中心都进行了假膜去除、使用人工泪液和维生素 A 软膏(8/9,90%)。6 个中心(67%)使用了联合抗生素皮质类固醇或皮质类固醇眼药水,3 个中心(33%)仅使用抗生素和防腐剂。如果需要,5 个中心(55%)使用睑球粘连环。羊膜移植从未系统地进行,仅根据临床病程进行。偶尔会使用全身皮质类固醇治疗(3/9,33%),并根据具体情况进行讨论。关于 SJS/TEN 急性阶段眼部管理实践的文献相对较少。局部或全身皮质类固醇治疗等特定治疗的作用尚未达成共识。防腐剂的使用,经常存在于滴眼剂中,对眼表有害,应加以限制。早期羊膜移植似乎很有前途。