Golabi Pegah, Gerber Lynn, Paik James M, Deshpande Rati, de Avila Leyla, Younossi Zobair M
Betty and Guy Beatty Center for Integrated Research, Inova Health System, Falls Church, VA, USA.
Center for Liver Disease, Department of Medicine, Inova Fairfax Hospital, Falls Church, VA, USA.
JHEP Rep. 2020 Aug 15;2(6):100171. doi: 10.1016/j.jhepr.2020.100171. eCollection 2020 Dec.
BACKGROUND & AIMS: Physical inactivity and sedentary lifestyle have contributed to the epidemic of obesity and non-alcoholic fatty liver disease (NAFLD). We assessed the association between physical activity, NAFLD, and sarcopenia, and their contributions to mortality.
Data from the National Health and Nutrition Examination Survey (NHANES) 1999-2004 with Linked Mortality file (through 2015) was utilised. NAFLD was determined by the US Fatty Liver Index in the absence of secondary causes of liver disease. Sarcopenia was defined using appendicular lean mass divided by body mass index by the Foundation for the National Institutes of Health criteria. Activity level was determined using standard self-reports. Publicly available imputed dual-energy X-ray absorptiometry data sets were used.
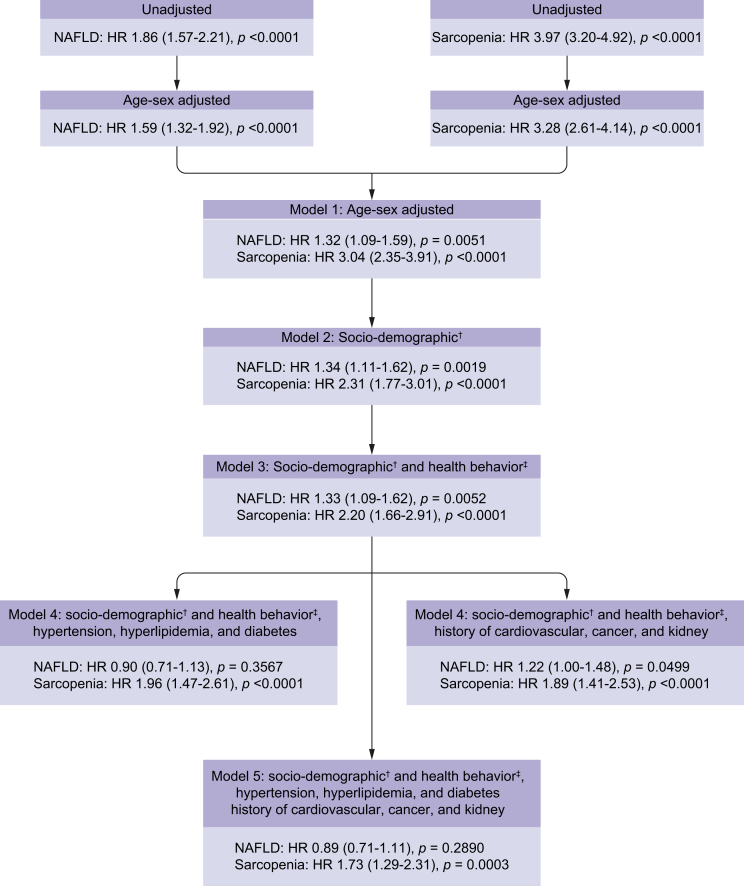
Of 4,611 NHANES participants (48.2% males; 72.5% White; mean age 45.9 years), NAFLD was present in 1,351 (29.3%), of whom 17.7% had sarcopenia. Of the NAFLD group, 46.3% was inactive, whilst intermediate and ideal physical activity rates were observed in 14.2% and 39.5%, respectively. Sarcopenia was significantly and inversely related to higher physical activity level, both amongst NAFLD (odds ratio [OR] = 0.45 [95% CI 0.30-0.69]) and non-NAFLD (OR = 0.51 [0.35-0.75]) groups. During a median follow-up of 13.5 years, a total of 586 subjects died, of whom 251 had NAFLD. Amongst those who died with NAFLD, 33.0% had sarcopenia and 54.3% were inactive. Compared with NAFLD without sarcopenia, NAFLD with sarcopenia was associated with a higher risk of all-cause (hazard ratio [HR] = 1.78 [1.16-2.73]), cardiac-specific (HR = 3.19 [1.17-8.74]), and cancer-specific mortality (HR = 2.12 [1.08-4.15]).
Inactivity is associated with presence of sarcopenia, whilst sarcopenia is associated with increased mortality amongst NAFLD patients. Sarcopenia should be a part of clinical assessment of patients with NAFLD. Treatment of NAFLD should include optimal management of sarcopenia.
Nonalcoholic fatty liver disease (NAFLD) and sarcopenia have similar pathophysiological profiles. Our data show that sarcopenia is associated with inactivity in subjects with NAFLD. The presence of sarcopenia in patients with NAFLD poses increased risk for all-cause and cardiac-specific mortality.
缺乏身体活动和久坐不动的生活方式导致了肥胖和非酒精性脂肪性肝病(NAFLD)的流行。我们评估了身体活动、NAFLD和肌肉减少症之间的关联,以及它们对死亡率的影响。
利用1999 - 2004年美国国家健康与营养检查调查(NHANES)的数据以及关联的死亡率文件(截至2015年)。在没有肝病继发原因的情况下,通过美国脂肪肝指数确定NAFLD。根据美国国立卫生研究院基金会的标准,用四肢瘦体重除以体重指数来定义肌肉减少症。通过标准的自我报告确定活动水平。使用公开可用的估算双能X线吸收法数据集。
在4611名NHANES参与者中(48.2%为男性;72.5%为白人;平均年龄45.9岁),1351人(29.3%)患有NAFLD,其中17.7%有肌肉减少症。在NAFLD组中,46.3%的人缺乏身体活动,而中等和理想身体活动率分别为14.2%和39.5%。在NAFLD组(优势比[OR]=0.45[95%可信区间0.30 - 0.69])和非NAFLD组(OR = 0.51[0.35 - 0.75])中,肌肉减少症与较高的身体活动水平均呈显著负相关。在中位随访13.5年期间,共有586名受试者死亡,其中251人患有NAFLD。在死于NAFLD的患者中,33.0%有肌肉减少症,54.3%缺乏身体活动。与没有肌肉减少症的NAFLD患者相比,伴有肌肉减少症的NAFLD患者全因死亡风险更高(风险比[HR]=1.78[1.16 - 2.73])、心脏特异性死亡风险更高(HR = 3.19[1.17 - 8.74])以及癌症特异性死亡风险更高(HR = 2.12[1.08 - 4.15])。
缺乏身体活动与肌肉减少症的存在相关,而肌肉减少症与NAFLD患者死亡率增加相关。肌肉减少症应成为NAFLD患者临床评估的一部分。NAFLD的治疗应包括对肌肉减少症的优化管理。
非酒精性脂肪性肝病(NAFLD)和肌肉减少症具有相似的病理生理特征。我们的数据表明,在NAFLD患者中,肌肉减少症与缺乏身体活动相关。NAFLD患者中肌肉减少症的存在会增加全因死亡和心脏特异性死亡的风险。