Department of Radiation Oncology, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, 0097, FCT10.6002, Houston, TX, 77030, USA.
MD Anderson Cancer Center UTHealth Graduate School of Biomedical Sciences, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
BMC Cancer. 2020 Sep 23;20(1):912. doi: 10.1186/s12885-020-07427-7.
The incidence of oropharyngeal squamous cell carcinoma (OPSCC) in the US is rapidly increasing, driven largely by the epidemic of human papillomavirus (HPV)-mediated OPSCC. Although survival for patients with HPV mediated OPSCC (HPV+ OPSCC) is generally better than that of patients with non-virally mediated OPSCC, this effect is not uniform. We hypothesized that tobacco exposure remains a critical modifier of survival for HPV+ OPSCC patients.
We conducted a retrospective analysis of 611 OPSCC patients with concordant p16 and HPV testing treated at a single institute (2002-2013). Survival analysis was performed using Kaplan-Meier analysis and Cox regression. Recursive partitioning analysis (RPA) was used to define tobacco exposure associated with survival (p < 0.05).
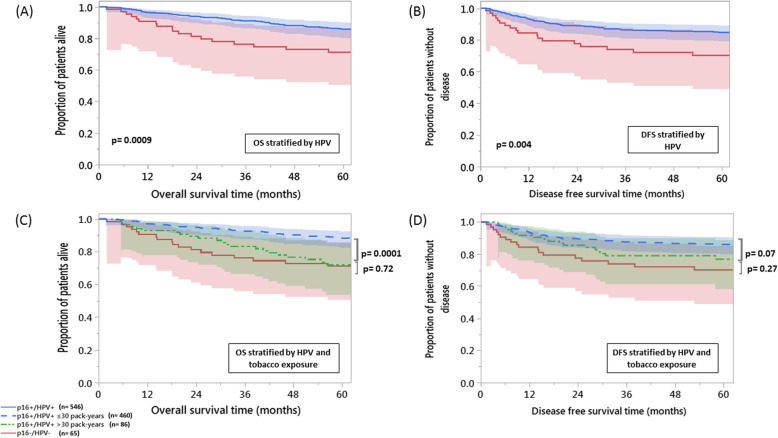
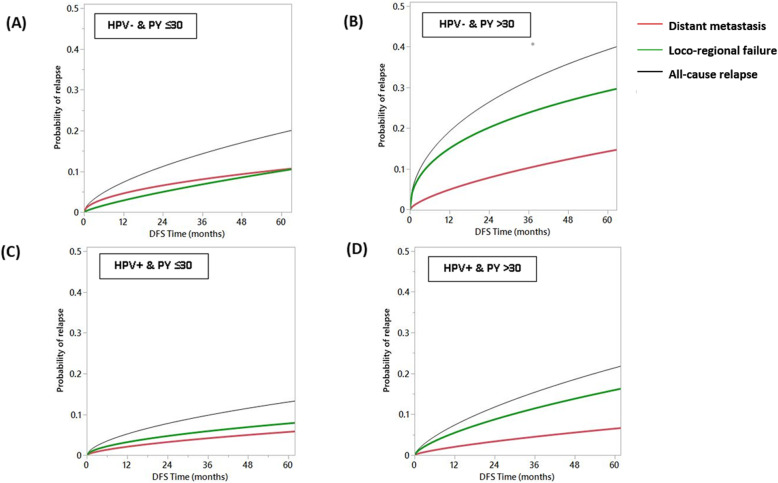
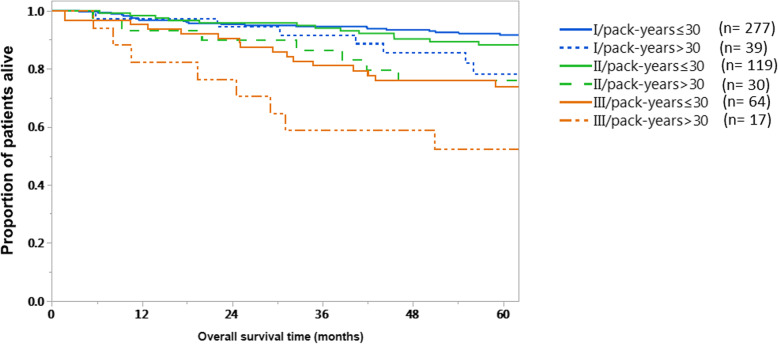
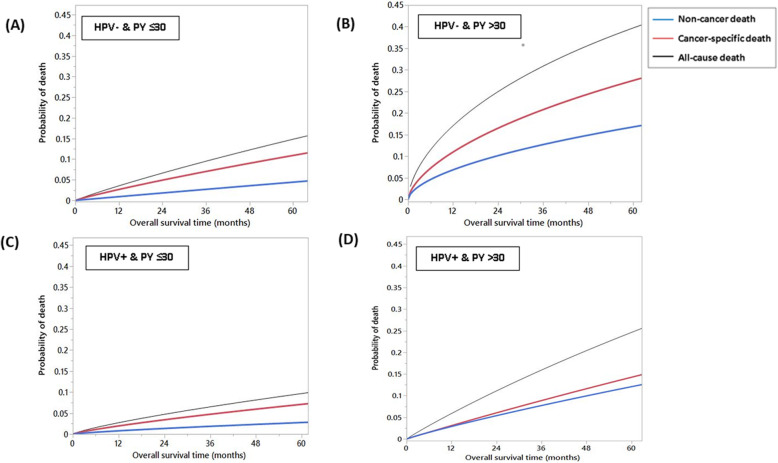
Tobacco exposure impacted overall survival (OS) for HPV+ patients on univariate and multivariate analysis (p = 0.002, p = 0.003 respectively). RPA identified 30 pack-years (PY) as a threshold at which survival became significantly worse in HPV+ patients. OS and disease-free survival (DFS) for HPV+ > 30 PY patients didn't differ significantly from HPV- patients (p = 0.72, p = 0.27, respectively). HPV+ > 30 PY patients had substantially lower 5-year OS when compared to their ≤30 PYs counterparts: 78.4% vs 91.6%; p = 0.03, 76% vs 88.3%; p = 0.07, and 52.3% vs 74%; p = 0.05, for stages I, II, and III (AJCC 8th Edition Manual), respectively.
Tobacco exposure can eliminate the survival benefit associated with HPV+ status in OPSCC patients. Until this effect can be clearly quantified using prospective datasets, de-escalation of treatment for HPV + OPSCC smokers should be avoided.
美国口咽鳞状细胞癌(OPSCC)的发病率迅速上升,主要是由 HPV 介导的 OPSCC 流行所致。尽管 HPV 介导的 OPSCC(HPV+ OPSCC)患者的生存率一般高于非病毒介导的 OPSCC 患者,但这种效果并非一致。我们假设,烟草暴露仍然是 HPV+ OPSCC 患者生存的关键修饰因素。
我们对一家机构(2002-2013 年)治疗的 611 例 p16 和 HPV 检测结果一致的 OPSCC 患者进行了回顾性分析。采用 Kaplan-Meier 分析和 Cox 回归进行生存分析。递归分区分析(RPA)用于定义与生存相关的烟草暴露(p<0.05)。
在单因素和多因素分析中,烟草暴露对 HPV+ 患者的总生存(OS)有影响(p=0.002,p=0.003)。RPA 确定 30 包年(PY)为 HPV+ 患者生存显著恶化的阈值。HPV+ >30 PY 患者的 OS 和无病生存(DFS)与 HPV- 患者无显著差异(p=0.72,p=0.27)。与 HPV+ ≤30 PY 患者相比,HPV+ >30 PY 患者的 5 年 OS 显著降低:78.4% vs 91.6%;p=0.03,76% vs 88.3%;p=0.07,52.3% vs 74%;p=0.05,分别用于 AJCC 第 8 版手册的 I、II 和 III 期。
烟草暴露可消除 HPV+ OPSCC 患者生存获益。在能够使用前瞻性数据集明确量化这种效果之前,应避免减少 HPV+ OPSCC 吸烟者的治疗。