Sitaram Bhartia Institute of Science and Research, Delhi, India.
BMC Pregnancy Childbirth. 2020 Sep 23;20(1):556. doi: 10.1186/s12884-020-03234-x.
In line with global trends, India has witnessed a sharp rise in caesarean section (CS) deliveries, especially in the private sector. Despite the urgent need for change, there are few published examples of private hospitals that have successfully lowered their CS rates. Our hospital, serving private patients too, had a CS rate of 79% in 2001. Care was provided by fee-for-service visiting consultant obstetricians without uniform clinical protocols and little clinical governance. Consultants attributed high CS rate to case-mix and maternal demand and showed little inclination for change. We attempted to reduce this rate with the objective of improving the quality of our care and demonstrating that CS could be safely lowered in the private urban Indian healthcare setting.
We hired full-time salaried consultants and began regular audit of CS cases. When this proved inadequate, we joined an improvement collaborative in 2011 and dedicated resources for quality improvement. We adopted practice guidelines, monitored outcomes by consultant, improved labour ward support, strengthened antenatal preparation, and moved to group practice among consultants.
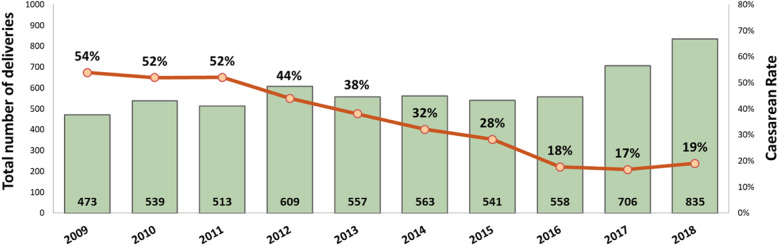
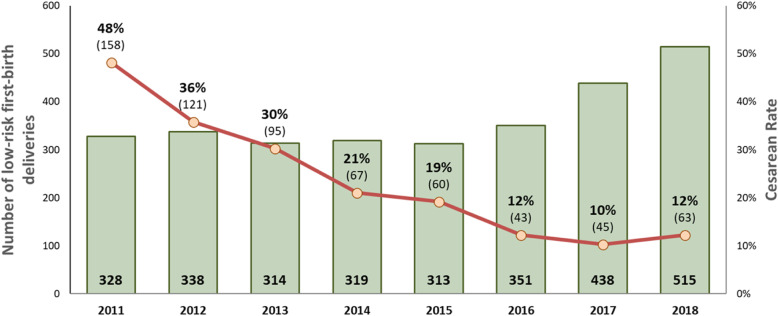
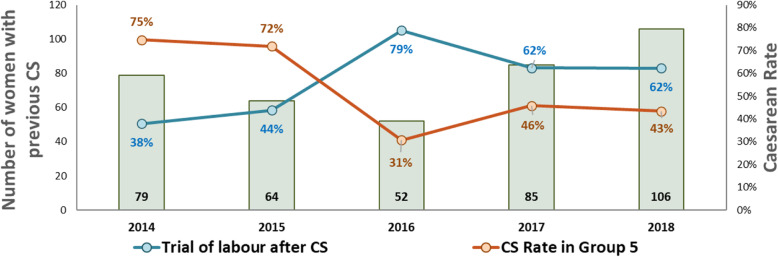
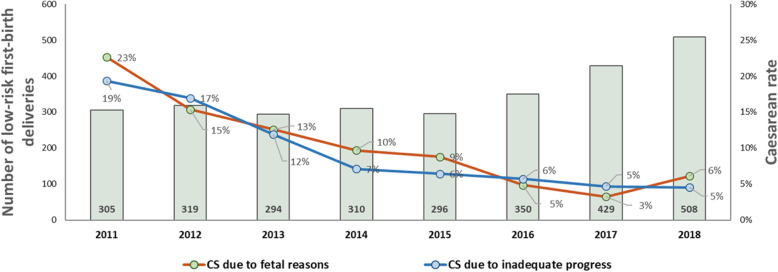
Guidelines ensured admissions in active labour and reduced CS (2011 to 2016) for foetal heart rate abnormalities (23 to 5%; p < 0.001) and delayed progress (19 to 6%; p < 0.001) in low-risk first-birth women. Antenatal preparation increased trial of labour, even among women with prior CS (28 to 79%; p < 0.001). Group practice reduced time pressure and stress, with a decline in CS (52 to 18%; p < 0.001) and low-risk first-birth CS (48 to 12%; p < 0.001). Similar CS rates were maintained in 2017 and 2018. Measures of perinatal harm including post-partum haemorrhage, 3rd-4th degree tears, shoulder dystocia, and Apgar < 7 at 5 min were within acceptable ranges (13, 3, 2% and 3 per thousand respectively in 2016-18,).
It is feasible to substantially reduce CS rate in private healthcare setting of a middle-income country like India. Ideas such as moving to full-time attachment of consultants, joining a collaborative, improving labour ward support, providing resources for data collection, and perseverance could be adopted by other hospitals in their own journey of moving towards a medically justifiable CS rate.
与全球趋势一致,印度的剖宫产(CS)分娩率,尤其是在私营部门,急剧上升。尽管迫切需要改变,但很少有发表的例子表明私营医院已经成功降低了 CS 率。我们的医院也为私人患者提供服务,2001 年的 CS 率为 79%。由按服务收费的顾问产科医生提供护理,没有统一的临床方案,也没有多少临床治理。顾问们将高 CS 率归因于病例组合和产妇需求,并且几乎没有改变的意愿。我们试图降低这一比率,目的是提高我们的护理质量,并证明在印度城市私立医疗保健环境中可以安全降低 CS 率。
我们聘请了全职受薪顾问,并开始对 CS 病例进行定期审核。当这证明是不够的,我们在 2011 年加入了一个改进合作,并专门为质量改进投入资源。我们采用了实践指南,通过顾问监测结果,改善产房支持,加强产前准备,并在顾问之间实行小组实践。
指南确保在活跃分娩时入院,并减少 CS(2011 年至 2016 年)用于胎心异常(23 至 5%;p<0.001)和低危初产妇进展延迟(19 至 6%;p<0.001)。产前准备增加了试产,即使是有先前 CS 史的妇女也是如此(28 至 79%;p<0.001)。小组实践减少了时间压力和紧张,CS 率下降(52 至 18%;p<0.001),低危初产妇 CS 率下降(48 至 12%;p<0.001)。2017 年和 2018 年保持了类似的 CS 率。包括产后出血、3 度-4 度撕裂、肩难产和 Apgar<5 分钟分别为 7 分的围产期伤害指标均在可接受范围内(2016-18 年分别为 13%、3%、2%和 3%)。
在印度这样的中等收入国家的私立医疗保健环境中,大幅度降低 CS 率是可行的。诸如全职顾问的加入、合作的加入、产房支持的改善、数据收集资源的提供和坚持不懈等想法,其他医院可以在自己的降低 CS 率的过程中借鉴。