Duke Clinical Research Institute, Duke University Medical Center, Durham, North Carolina.
Division of Nephrology, Duke University Medical Center, Durham, North Carolina.
Clin J Am Soc Nephrol. 2020 Nov 6;15(11):1622-1630. doi: 10.2215/CJN.07920520. Epub 2020 Sep 23.
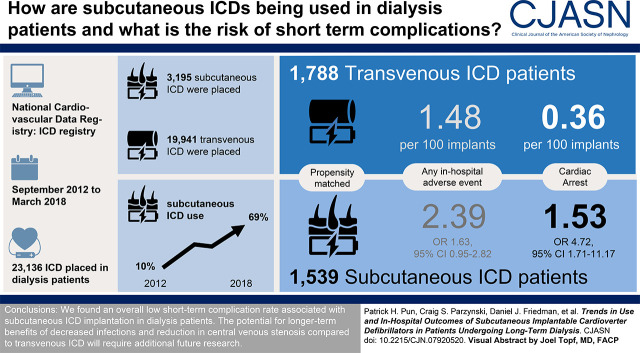
Patients on dialysis are at high risk of complications related to implantable cardioverter defibrillator (ICD) implantation; use of subcutaneous ICDs may be preferred over transvenous devices due to lower risk of bloodstream infection and interference with vascular access sites. We evaluated trends in use and in-hospital outcomes of subcutaneous compared with transvenous ICDs among patients on dialysis in the United States.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: Retrospective analysis of ICD implants from 2012 to 2018 among patients on dialysis reported to the National Cardiovascular Data Registry ICD Registry, a nationally representative US ICD Registry. We examined overall trends in subcutaneous ICD adoption as a proportion of all eligible ICD implants among patients on dialysis and then compared in-hospital outcomes between eligible subcutaneous ICD and transvenous ICD recipients using inverse probability of treatment weighting.
Of the 23,136 total ICD implants in patients on dialysis during the study period, 3195 (14%) were subcutaneous ICDs. Among eligible first-time ICD recipients on dialysis, the proportion of subcutaneous ICDs used increased yearly from 10% in 2012 to 69% in 2018. In propensity score-weighted analysis of 3327 patients, compared with transvenous ICDs, patients on dialysis receiving subcutaneous ICDs had a higher rate of in-hospital cardiac arrest (2% versus 0.4%, =0.002), but there was no significant difference in total in-hospital complications (2% versus 1%, =0.08), all-cause death, or length of hospital stay.
The utilization of subcutaneous ICDs among US patients on dialysis has been steadily increasing. The overall risk of short-term complications is low and comparable with transvenous ICDs, but higher risks of in-hospital cardiac arrest merits closer monitoring and further investigation.
This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2020_09_23_CJN07920520.mp3.
接受透析治疗的患者发生与植入式心脏复律除颤器(ICD)植入相关并发症的风险较高;由于血流感染风险较低且不会干扰血管通路部位,皮下 ICD 可能优于经静脉装置。我们评估了美国接受透析治疗的患者中皮下 ICD 与经静脉 ICD 的使用趋势及其住院结局。
设计、地点、参与者和测量:对 2012 年至 2018 年向全国心血管数据注册 ICD 登记处报告的接受透析治疗的患者 ICD 植入病例进行回顾性分析,该登记处是一个具有全国代表性的美国 ICD 登记处。我们检查了透析患者中皮下 ICD 作为所有合格 ICD 植入物比例的总体采用趋势,然后使用治疗倾向评分加权法比较了合格皮下 ICD 和经静脉 ICD 接受者的住院结局。
在研究期间,23136 例接受透析治疗的患者中,共有 3195 例(14%)接受了皮下 ICD 治疗。在首次接受透析治疗的合格 ICD 患者中,每年皮下 ICD 的使用比例从 2012 年的 10%增加到 2018 年的 69%。在对 3327 例患者进行倾向评分加权分析中,与经静脉 ICD 相比,接受皮下 ICD 的透析患者住院期间发生心脏骤停的比例更高(2%比 0.4%,=0.002),但总住院并发症(2%比 1%,=0.08)、全因死亡率或住院时间无显著差异。
美国接受透析治疗的患者中皮下 ICD 的使用稳步增加。短期并发症的总体风险较低,与经静脉 ICD 相当,但住院期间心脏骤停的风险较高,需要更密切的监测和进一步研究。
本文包含播客,网址为 https://www.asn-online.org/media/podcast/CJASN/2020_09_23_CJN07920520.mp3。