Department of Urology, University of Wisconsin School of Medicine and Public Health, 1685 Highland Ave., Madison, WI 53705, USA; Cancer Biology Graduate Program, University of Wisconsin-Madison, Wisconsin Institute for Medical Research, 1111 Highland Ave., Madison, WI 53705, USA; Carbone Cancer Center, University of Wisconsin School of Medicine and Public Health, 600 Highland Ave., Madison, WI 53705, USA.
Department of Urology, University of Wisconsin School of Medicine and Public Health, 1685 Highland Ave., Madison, WI 53705, USA; Carbone Cancer Center, University of Wisconsin School of Medicine and Public Health, 600 Highland Ave., Madison, WI 53705, USA; George M. O'Brien Research Center of Excellence, University of Wisconsin School of Medicine and Public Health, 1685 Highland Ave., Madison, WI 53705, USA.
Neoplasia. 2020 Nov;22(11):566-575. doi: 10.1016/j.neo.2020.09.002. Epub 2020 Sep 25.
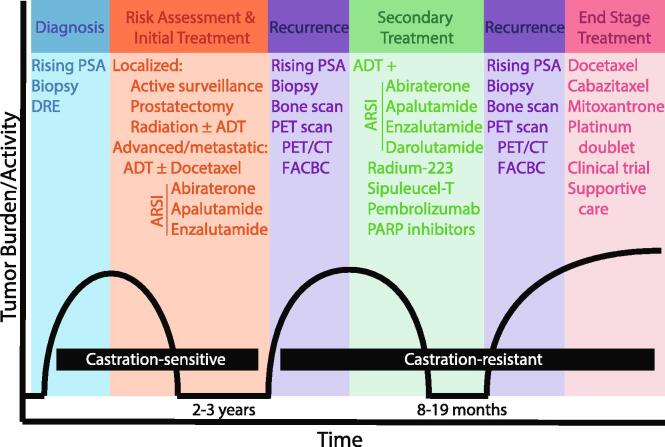
Castration-resistant prostate cancer (CRPC) occurs when prostate cancer (CaP) progresses under therapy-induced castrate conditions. Several mechanisms have been proposed to explain this acquired resistance, many of which are driven by androgen receptor (AR). Recent findings, however, sub-classified CRPC by downregulation/absence of AR in certain subtypes that consequently do not respond to anti-androgen therapies. To highlight the significance of CRPC sub-classification, we reviewed the development and treatment of CRPC, AR downregulation in CRPC, and summarized recent reports on the prevalence of CRPC subtypes.
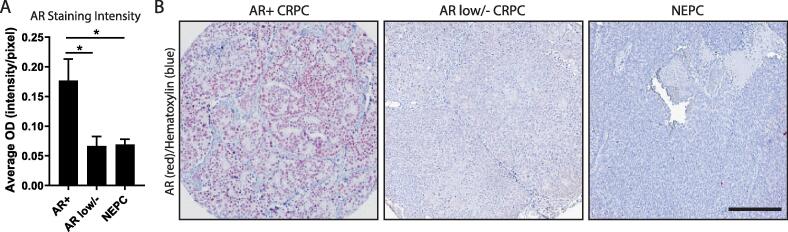
Using a medline-based literature search, we reviewed mechanisms of CRPC development, current treatment schemes, and assessed the prevalence of AR low/negative subtypes of CRPC. Additionally, we performed immunohistochemical staining on human CRPC specimens to quantify AR expression across CRPC subtypes.
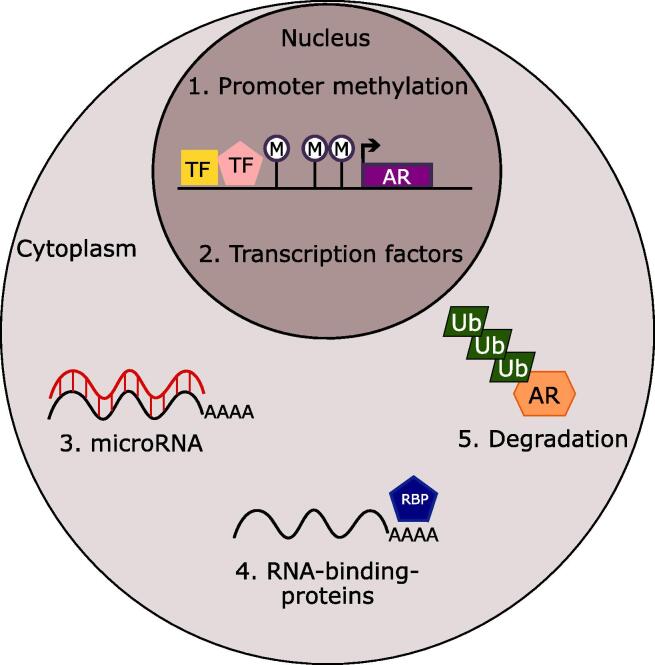
In the majority of cases, CRPC continues to rely on AR signaling, which can be augmented in castrate-conditions through a variety of mechanisms. However, recently low/negative AR expression patterns were identified in a significant proportion of patient samples from a multitude of independent studies. In these AR low/negative cases, we postulated that AR protein may be downregulated by (1) promoter methylation, (2) transcriptional regulation, (3) post-transcriptional regulation by microRNA or RNA-binding-proteins, or (4) post-translational ubiquitination-mediated degradation.
Here, we discussed mechanisms of CRPC development and summarized the overall prevalence of CRPC subtypes; interestingly, AR low/negative CRPC represented a considerable proportion of diagnoses. Because these subtypes cannot be effectively treated with AR-targeted therapeutics, a better understanding of AR low/negative subtypes could lead to better treatment strategies and increased survival.
当前列腺癌(CaP)在治疗诱导的去势条件下进展时,会发生去势抵抗性前列腺癌(CRPC)。已经提出了几种机制来解释这种获得性耐药,其中许多机制是由雄激素受体(AR)驱动的。然而,最近的发现将 CRPC 分为亚类,某些亚类的 AR 下调/缺失,因此对抗雄激素治疗没有反应。为了强调 CRPC 亚类分类的意义,我们回顾了 CRPC 的发展和治疗、CRPC 中 AR 下调以及总结了最近关于 CRPC 亚型患病率的报告。
我们使用基于 medline 的文献搜索,回顾了 CRPC 发展的机制、当前的治疗方案,并评估了 AR 低/阴性 CRPC 亚型的患病率。此外,我们对人类 CRPC 标本进行了免疫组织化学染色,以定量评估 CRPC 亚型中 AR 的表达。
在大多数情况下,CRPC 仍然依赖于 AR 信号转导,在去势条件下,通过多种机制可以增强 AR 信号转导。然而,最近在大量独立研究的患者样本中发现了相当一部分低/阴性 AR 表达模式。在这些 AR 低/阴性病例中,我们推测 AR 蛋白可能通过以下机制下调:(1)启动子甲基化,(2)转录调控,(3)microRNA 或 RNA 结合蛋白的转录后调控,或(4)翻译后泛素化介导的降解。
在这里,我们讨论了 CRPC 发展的机制,并总结了 CRPC 亚型的总体患病率;有趣的是,AR 低/阴性 CRPC 代表了相当大比例的诊断。由于这些亚型不能用 AR 靶向治疗有效治疗,因此更好地了解 AR 低/阴性亚型可能会导致更好的治疗策略和生存率提高。