Kuribara Tadao, Ichikawa Tatsuo, Osa Kiyoshi, Inoue Takeshi, Ono Satoshi, Asanuma Kozo, Kaneko Shiori, Sano Takayuki, Shigeyoshi Itaru, Matsubara Kouta, Irie Naoko, Iai Akira, Shinobi Tetsuya, Ishizu Hideki, Miura Katsuhiro
Department of Surgery, Saitama Cooperative Hospital, 1317 Kizoro, Kawaguchi-shi, Saitama, 333-0831, Japan.
Department of Internal Medicine, Saitama Cooperative Hospital, 1317 Kizoro, Kawaguchi-shi, Saitama, Japan.
Surg Case Rep. 2020 Sep 29;6(1):228. doi: 10.1186/s40792-020-00997-5.
Pancreaticoduodenectomy (PD) is rarely performed for pancreatic cancer with hepatic arterial invasion owing to its poor prognosis and high surgical risks. Although there has been a recent increase in the reports of PD combined with hepatic arterial resection due to improvements in disease prognosis and operative safety, PD with major arterial resection and reconstruction is still considered a challenging treatment.
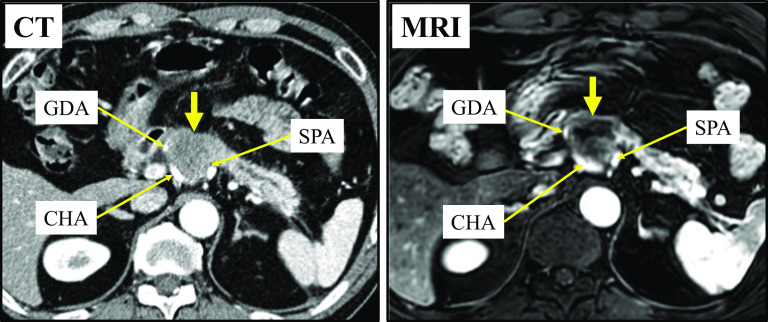
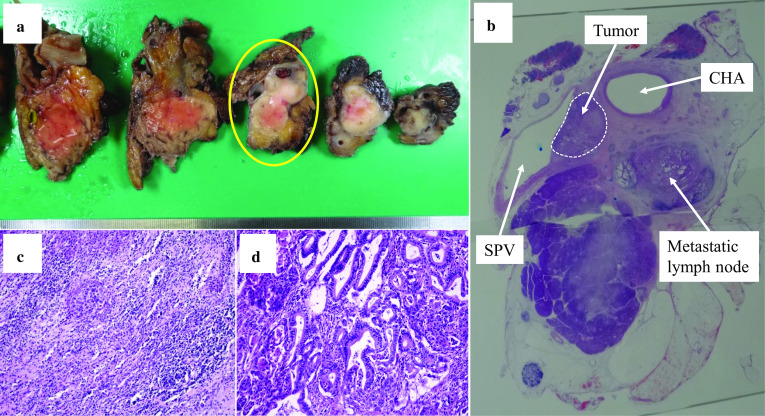
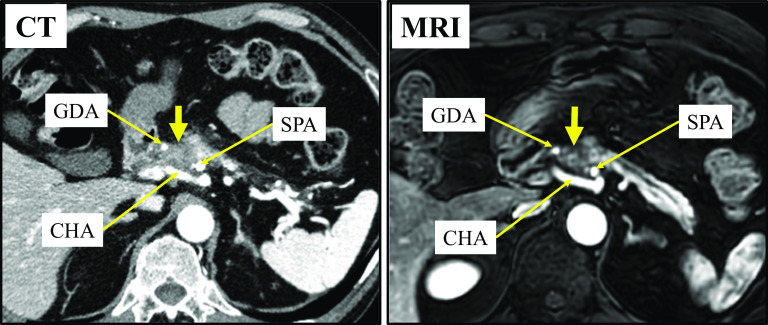
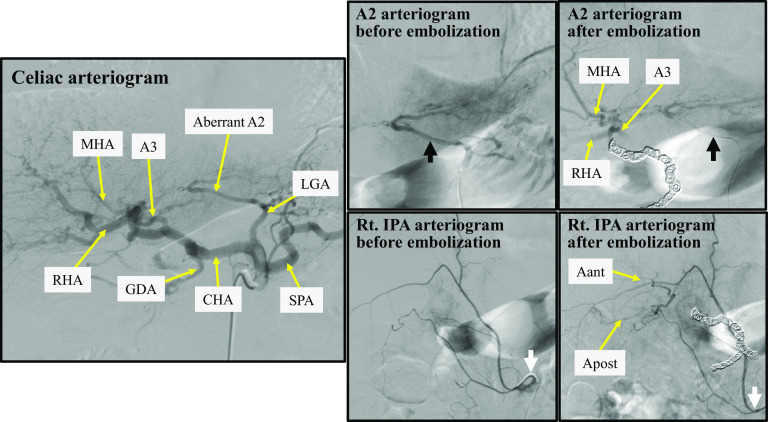
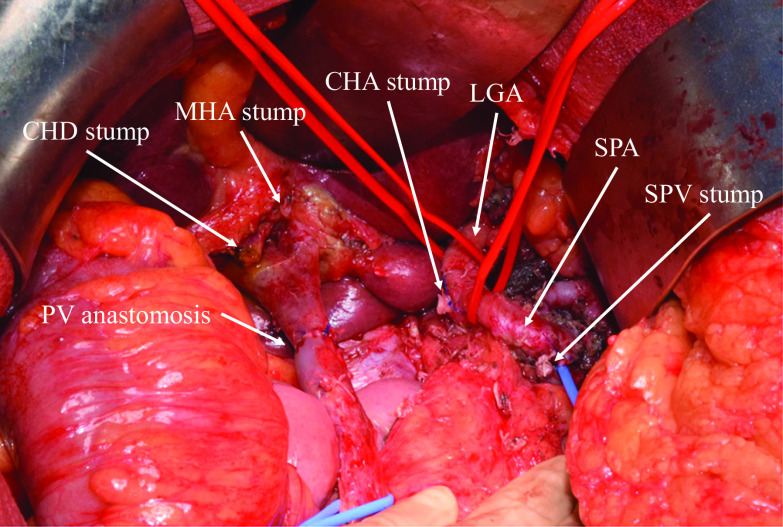
A 61-year-old man with back pain was diagnosed with pancreatic head and body cancer. Although distant metastasis was not confirmed, the tumor had extensively invaded the hepatic artery; therefore, we diagnosed the patient with locally advanced unresectable pancreatic cancer. After gemcitabine plus nab-paclitaxel (GnP) therapy, the tumor considerably decreased in size from 35 to 20 mm. Magnetic resonance imaging revealed a gap between the tumor and the hepatic artery. Tumor marker levels returned to their normal range, and we decided to perform conversion surgery. In this case, an artery of liver segment 2 (A2) had branched from the left gastric artery; therefore, we decided to preserve A2 and perform PD combined with hepatic arterial resection without reconstruction. After four cycles of GnP therapy, we performed hepatic arterial embolization to prevent postoperative ischemic complications prior to surgery. Immediately after embolization, collateral arterial blood flow to the liver was observed. Operation was performed 19 days after embolization. Although there was a temporary increase in liver enzyme levels and an ischemic region was found near the surface of segment 8 of the liver after surgery, no liver abscess developed. The postoperative course was uneventful, and S-1 was administered for a year as adjuvant chemotherapy. The patient is currently alive without any ischemic liver events and cholangitis and has not experienced recurrence in the past 4 years since the surgery.
In PD for pancreatic cancer with hepatic arterial invasion, if a part of the hepatic artery is aberrant and can be preserved, combined resection of the common and proper hepatic artery without reconstruction might be feasible for both curability and safety.
由于预后较差且手术风险高,胰十二指肠切除术(PD)很少用于治疗侵犯肝动脉的胰腺癌。尽管近年来由于疾病预后和手术安全性的改善,PD联合肝动脉切除术的报道有所增加,但进行主要动脉切除和重建的PD仍然被认为是一种具有挑战性的治疗方法。
一名61岁背痛男性被诊断为胰头和胰体癌。虽然未证实有远处转移,但肿瘤已广泛侵犯肝动脉;因此,我们将该患者诊断为局部晚期不可切除胰腺癌。在吉西他滨加纳米白蛋白结合型紫杉醇(GnP)治疗后,肿瘤大小从35毫米大幅缩小至20毫米。磁共振成像显示肿瘤与肝动脉之间有间隙。肿瘤标志物水平恢复到正常范围,我们决定进行转化手术。在该病例中,肝2段动脉(A2)从胃左动脉分支;因此,我们决定保留A2并进行不重建的PD联合肝动脉切除术。在四个周期的GnP治疗后,我们在手术前进行了肝动脉栓塞以预防术后缺血性并发症。栓塞后立即观察到肝脏的侧支动脉血流。栓塞后19天进行了手术。虽然术后肝酶水平暂时升高,且在肝8段表面附近发现了一个缺血区域,但未发生肝脓肿。术后病程平稳,给予S-1辅助化疗一年。患者目前存活,无任何肝脏缺血事件和胆管炎,自手术以来的4年中未出现复发。
在治疗侵犯肝动脉的胰腺癌的PD中,如果肝动脉的一部分走行异常且可保留,则不进行重建的肝总动脉和肝固有动脉联合切除术在可治愈性和安全性方面可能是可行的。