Wheeler David C, James June, Patel Dipesh, Viljoen Adie, Ali Amar, Evans Marc, Fernando Kevin, Hicks Debbie, Milne Nicola, Newland-Jones Philip, Wilding John
University College London, London, UK.
University Hospitals of Leicester NHS Trust, University of Leicester, Leicester, UK.
Diabetes Ther. 2020 Dec;11(12):2757-2774. doi: 10.1007/s13300-020-00930-x. Epub 2020 Sep 29.
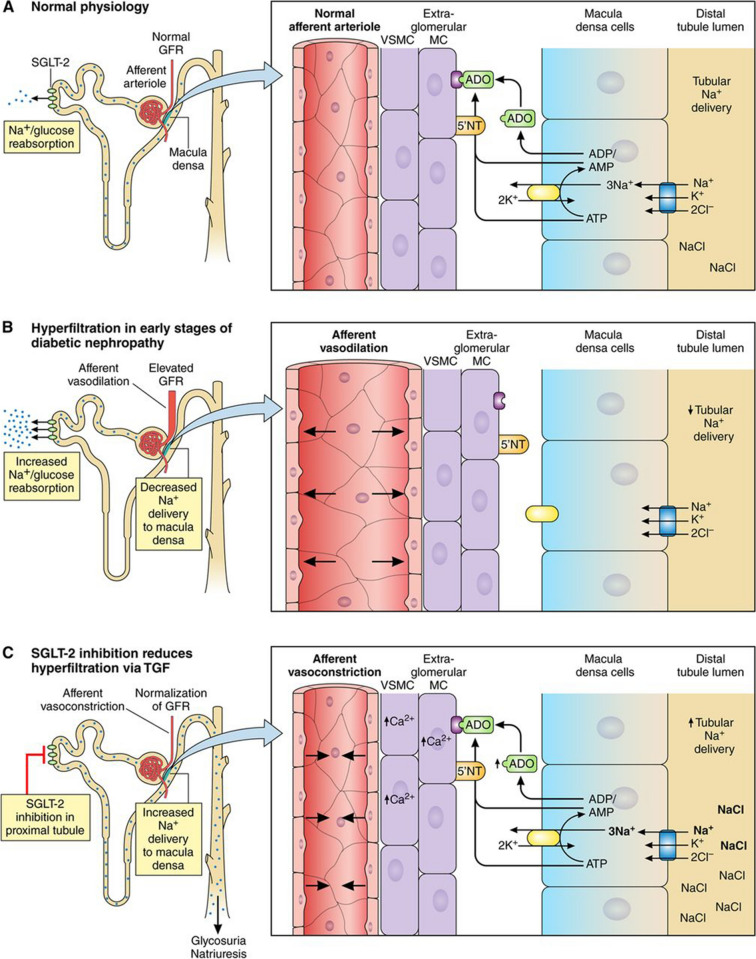
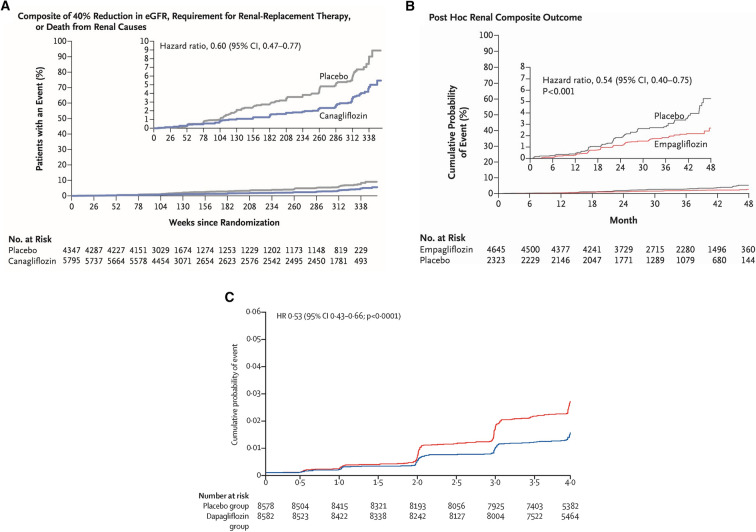
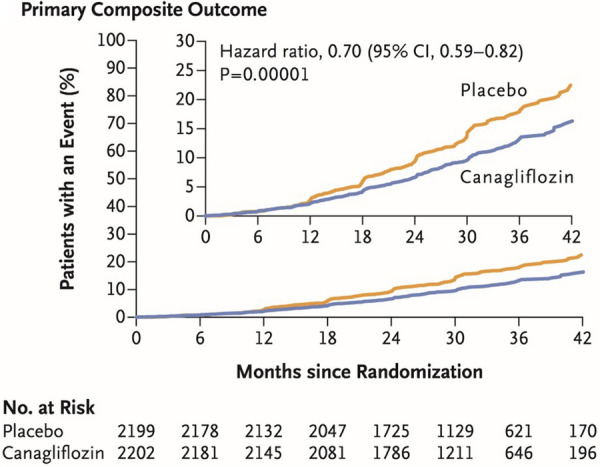
Diabetic kidney disease (DKD) is a topic of increasing concern among clinicians involved in the management of type 2 diabetes mellitus (T2DM). It is a progressive and costly complication associated with increased risk of adverse cardiovascular (CV) and renal outcomes and mortality. Ongoing monitoring of the estimated glomerular filtration (eGFR) rate alongside the urine albumin:creatinine ratio (ACR) is recommended during regular T2DM reviews to enable a prompt DKD diagnosis or to assess disease progression, providing an understanding of adverse risk for each individual. Many people with DKD will progress to end-stage kidney disease (ESKD), requiring renal replacement therapy (RRT), typically haemodialysis or kidney transplantation. A range of lifestyle and pharmacological interventions is recommended to help lower CV risk, slow the advancement of DKD and prevent or delay the need for RRT. Emerging evidence concerning sodium-glucose co-transporter-2 inhibitor (SGLT2i) agents suggests a role for these medicines in slowing eGFR decline, enabling regression of albuminuria and reducing progression to ESKD. Improvements in renal end points observed in SGLT2i CV outcome trials (CVOTs) highlighted the possible impact of these agents in the management of DKD. Data from the canagliflozin CREDENCE trial (Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation) have since demonstrated the effectiveness of this medicine in reducing the risk of kidney failure and CV events in a population comprising individuals with T2DM and renal disease. CREDENCE was the first SGLT2i study to examine renal outcomes as the primary end point. Real-world studies have reaffirmed these outcomes in routine clinical practice. This article summarises the evidence regarding the use of SGLT2i medicines in slowing the progression of DKD and examines the possible mechanisms underpinning the renoprotective effects of these agents. The relevant national and international guidance for monitoring and treatment of DKD is also highlighted to help clinicians working to support this vulnerable group.
糖尿病肾病(DKD)是参与2型糖尿病(T2DM)管理的临床医生日益关注的话题。它是一种渐进性且代价高昂的并发症,与不良心血管(CV)和肾脏结局风险增加以及死亡率上升相关。在定期的T2DM复查期间,建议同时持续监测估算肾小球滤过率(eGFR)以及尿白蛋白与肌酐比值(ACR),以便能及时诊断DKD或评估疾病进展,从而了解每个个体的不良风险。许多DKD患者会进展至终末期肾病(ESKD),需要肾脏替代治疗(RRT),通常是血液透析或肾脏移植。建议采取一系列生活方式和药物干预措施,以帮助降低CV风险、减缓DKD进展并预防或推迟RRT的需求。关于钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)药物的新证据表明,这些药物在减缓eGFR下降、使蛋白尿消退以及减少进展至ESKD方面发挥着作用。在SGLT-2i心血管结局试验(CVOT)中观察到的肾脏终点改善突出了这些药物在DKD管理中的潜在影响。卡格列净CREDENCE试验(卡格列净与糖尿病合并已确诊肾病临床评估中的肾脏事件)的数据此后证明了该药物在降低患有T2DM和肾病的人群中发生肾衰竭和CV事件风险方面的有效性。CREDENCE是首个将肾脏结局作为主要终点进行研究的SGLT2i研究。真实世界研究在常规临床实践中再次证实了这些结果。本文总结了关于使用SGLT-2i药物减缓DKD进展的证据,并探讨了这些药物肾脏保护作用的潜在机制。还强调了DKD监测和治疗的相关国家和国际指南,以帮助临床医生为这一弱势群体提供支持。