Trauma Unit, Kantonsspital Aarau, Tellstrasse 25, 5001, Aarau, Switzerland.
Division of Neuroradiology, Department of Radiology, Kantonsspital Aarau, Tellstrasse 25, 5001, Aarau, Switzerland.
Eur J Trauma Emerg Surg. 2022 Apr;48(2):921-931. doi: 10.1007/s00068-020-01502-1. Epub 2020 Sep 30.
The indication of whole body computed tomography (WBCT) in the emergency treatment of trauma is still under debate. We were interested in the detailed information gain obtained from WBCT following standardized conventional imaging (CI).
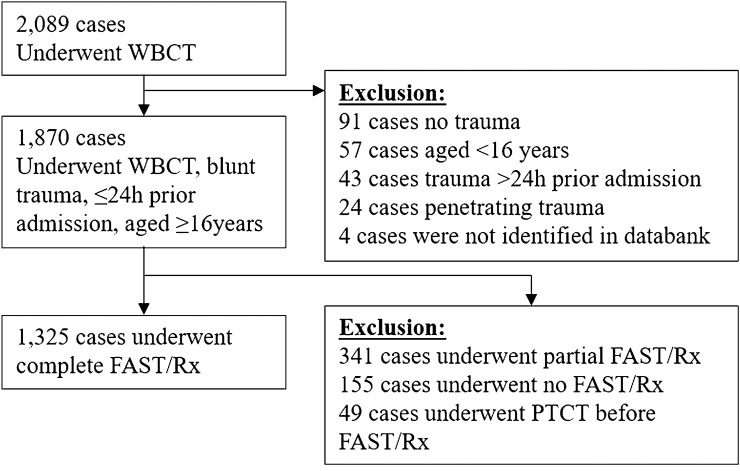
Prospective study including all emergency trauma centre patients examined by CI (focused assessment of sonography in trauma, chest and pelvic X-ray) followed by WBCT from 2011 to 2017. Radiology reports were compared per patient for defined body regions for number and severity of injuries (Abbreviated Injury Scale, AIS; Injury Severity Score, ISS), incidental findings and treatment consequences (Wilcoxon signed rank test, Spearman rho, Chi-square).
1271 trauma patients (ISS 11.3) were included in this study. WBCT detected more injury findings than CI in the equivalent body regions (1.8 vs. 0.6; p < 0.001). In 44.4% of cases at least one finding was missed by CI alone. Compared to WBCT, injury severity of specified body regions was underestimated by CI on average by an AIS of 1.9 (p < 0.001). In 22.0% of cases injury severity increased by an AIS ≥ 2 following WBCT. In 16.8% of patients additional injury findings resulted in a change of treatment (number needed to profit, NNP = 6 patients): NNP decreased from 25 for patients with an ISS < 7 up to nearly 2 for patients with an ISS > 25 at final evaluation, thereby demonstrating a significant improvement in the NNP with increasing ISS (rho = 0.33, p < 0.001). Moreover, WBCT in 88.4% of patients identified ≥ 1 incidental finding (mean 3.4) vs. 28.9% by CI only (p < 0.001). Overall, WBCT had treatment consequences in 31.9% of cases (NNP = 3.1).
The application of WBCT in addition to CI in the emergency treatment of trauma had therapy consequences for almost every third patient. On the other hand, WBCT appeared not to be indicated (ISS < 8) in at least 2/5 of patients.
全身计算机断层扫描(WBCT)在创伤急救中的应用仍存在争议。我们对接受标准化常规影像学(包括创伤超声重点评估、胸部和骨盆 X 线检查)后行 WBCT 所获得的详细信息感兴趣。
这是一项前瞻性研究,纳入了 2011 年至 2017 年间所有在我院接受常规影像学检查(包括创伤超声重点评估、胸部和骨盆 X 线检查)后行 WBCT 的创伤中心患者。对每位患者的特定身体区域的放射学报告进行比较,以评估损伤的数量和严重程度(损伤严重程度评分,ISS)、偶然发现和治疗后果(Wilcoxon 符号秩检验、Spearman rho、卡方检验)。
本研究共纳入 1271 例创伤患者(ISS 为 11.3)。WBCT 在等效身体区域检测到的损伤发现比 CI 多(1.8 比 0.6;p<0.001)。在 44.4%的情况下,CI 单独检查至少漏诊了一个损伤发现。与 WBCT 相比,CI 平均低估了指定身体区域的损伤严重程度 1.9 个 AIS 等级(p<0.001)。在 22.0%的情况下,WBCT 后损伤严重程度增加了 AIS≥2 个等级。在 16.8%的患者中,由于其他损伤发现,治疗方法发生了变化(需要治疗的患者数,NNP=6 例):ISS<7 的患者 NNP 从 25 例降至几乎 2 例,ISS>25 的患者 NNP 从 25 例降至几乎 2 例,表明随着 ISS 的增加,NNP 显著改善(rho=0.33,p<0.001)。此外,WBCT 在 88.4%的患者中发现了≥1 个偶然发现(平均 3.4 个),而仅在 28.9%的患者中发现了偶然发现(p<0.001)。总体而言,WBCT 在 31.9%的情况下具有治疗后果(NNP=3.1)。
在创伤急救中,除了 CI 之外,还应用 WBCT 治疗,几乎每 3 个患者中就有 1 个有治疗后果。另一方面,在至少 2/5的患者中,WBCT 似乎不是必需的(ISS<8)。