Kim Sollip, Yoo Soo Jin, Chang Jeonghyun
Laboratory Medicine, Inje University, Ilsan Paik Hospital, Goyang 10380, Korea.
Laboratory Medicine, Inje University, Sanggye Paik Hospital, Seoul 10757, Korea.
Medicina (Kaunas). 2020 Sep 28;56(10):507. doi: 10.3390/medicina56100507.
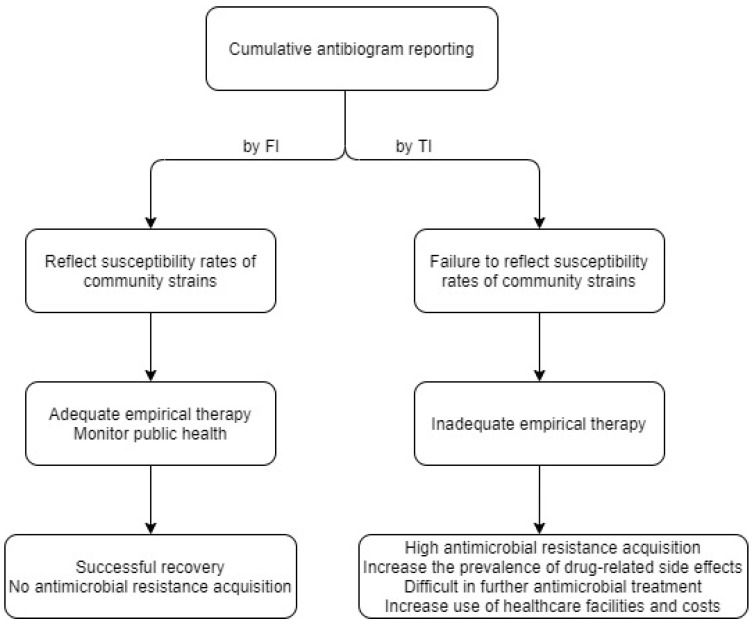
For proper antimicrobial therapy, cumulative antibiograms should be representative of geographic region and be accurate. Clinical and Laboratory Standards Institute (CLSI) guidelines recommend that only the first isolates (FI) of a species per patient are used when reporting cumulative antibiograms. However, >50% of hospitals in the United States report antibiograms of all isolates. We compared antibiograms from the FI with those from total isolates (TI). Antimicrobial data of all isolates identified in the Microbiology unit of Ilsan Paik Hospital in 2019 were retrospectively acquired from the hospital information system. The susceptibility rates to antimicrobials of , , , , , , and were analyzed by FI and TI, respectively. Isolate counts and susceptibility rates of each species for the reported antimicrobials were compared. The numbers of isolates by FI/TI were as follows: 1824/2692 , 480/1611 , and 662/1306 , and 407/953 for gram-negative bacteria and 649/1364 , 211/313 , and 323/394 for gram-positive bacteria. All antimicrobial agents showed higher susceptibility rates when calculated as FI than as TI in gram-negative bacteria except colistin: 3.7% for , 14.5% for , 8.3% for , and 7.9% for . In , 8/11 antimicrobial agents revealed higher susceptibility rates for FI than for TI. and showed lower susceptibility rates for 7/10 antimicrobial agents for FI than for TI. The oxacillin susceptibility rates of were 36.6%/30.2% with FI/TI and vancomycin susceptibility rates for were 54.1% and 49.5%, respectively. When comparing cumulative antibiograms by FI with TI using real-world data, there is a large gap for critical species requiring hospital infection control. Although FI calculation is difficult, antibiograms must be calculated as FI for proper preemptive antimicrobial therapy because FI provides proper antimicrobial susceptibility data.
为了进行恰当的抗菌治疗,累积抗菌谱应能代表所在地理区域且准确无误。临床和实验室标准协会(CLSI)指南建议,在报告累积抗菌谱时,每位患者每种细菌仅使用首次分离株(FI)。然而,美国超过50%的医院报告所有分离株的抗菌谱。我们比较了FI的抗菌谱与全部分离株(TI)的抗菌谱。回顾性地从医院信息系统获取了2019年一山白医院微生物科鉴定出的所有分离株的抗菌数据。分别分析了FI和TI对、、、、、、和的抗菌药物敏感性率。比较了每种细菌对报告抗菌药物的分离株数量和敏感性率。FI/TI的分离株数量如下:革兰阴性菌分别为1824/2692、480/1611、662/1306和407/953,革兰阳性菌分别为649/1364、211/313和323/394。除黏菌素外,在革兰阴性菌中,所有抗菌药物按FI计算时的敏感性率均高于按TI计算时的敏感性率:对为3.7%,对为14.5%,对为8.3%,对为7.9%。在中,11种抗菌药物中有8种FI的敏感性率高于TI。和中,10种抗菌药物中有7种FI的敏感性率低于TI。金黄色葡萄球菌的苯唑西林敏感性率FI/TI分别为36.6%/30.2%,万古霉素敏感性率分别为54.1%和49.5%。当使用实际数据比较FI与TI的累积抗菌谱时,对于需要医院感染控制的关键菌种存在很大差异。尽管计算FI很困难,但为了进行恰当的预防性抗菌治疗,抗菌谱必须按FI计算,因为FI能提供恰当的抗菌药物敏感性数据。