Department of Radiation Oncology, Tata Medical Center, Kolkata, India.
Trials. 2020 Sep 30;21(1):819. doi: 10.1186/s13063-020-04751-y.
Hypofractionated radiotherapy is the current standard for adjuvant radiotherapy across many centres. Further hypofractionation may be possible but remains to be investigated in non-Caucasian populations with more advanced disease, with a higher proportion of patients requiring mastectomy as well as tumour bed boost. We are reporting the design of randomized controlled trial testing the hypothesis that a 1-week (5 fractions) regimen of radiotherapy will be non-inferior to a standard 3-week (15 fractions) schedule.
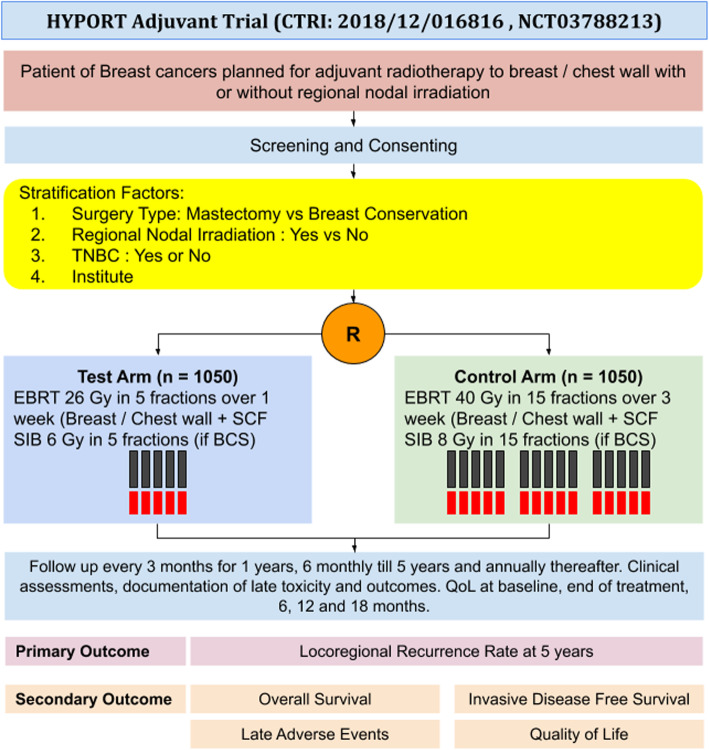
We describe a multicentre, randomized controlled trial recruiting patients at large academic centres across India. Patients without distant metastases who merit adjuvant radiotherapy will be eligible for inclusion in the study. Patients in the control arm will receive adjuvant radiotherapy to the breast or chest wall (with/without regional nodes) to a dose of 40 Gy/15 fractions/3 weeks, while those in the experimental arm will receive a dose of 26 Gy/5 fractions/1 week (to the same volume). The use of a simultaneous integrated boost (dose of 8 Gy and 6 Gy, respectively) is allowed in patients who have undergone breast conservation. A sample size of 2100 patients provides an 80% power to detect a non-inferiority of 3% in the 5-year locoregional recurrence rate with a one-sided type I error of 2.5%, assuming that the locoregional recurrence rate in the control arm is 5% at 5 years (corresponding to a hazard ratio of 1.63). Patients will be recruited over a period of 5 years and followed up for a further 5 years thereafter.
If a five-fraction regimen of breast cancer is proven to be non-inferior, this will result in a significant improvement in the access to radiotherapy, as well as reduced costs of treatment. The trial gives an opportunity to standardize and quality-assure radiotherapy practices across the nation at the same time. Along with the results of the FAST-Forward trial, the safety of this intervention in advanced node-positive disease requiring regional nodal radiation will be established.
The trial has been registered at the Clinical Trial Registry of India (CTRI) vide registration number: CTRI/2018/12/016816 (December 31, 2018) as well as the ClinicalTrial.gov website at NCT03788213 (December 28, 2018).
在许多中心,分割放疗是辅助放疗的当前标准。进一步的分割可能是可行的,但仍需在疾病程度更高、更多患者需要乳房切除术和肿瘤床加量放疗的非高加索人群中进行研究。我们报告了一项随机对照试验的设计,该试验检验了以下假设:一周(5 个疗程)的放疗方案与标准的三周(15 个疗程)方案相比不劣效。
我们描述了一项多中心、随机对照试验,该试验在印度的大型学术中心招募患者。没有远处转移且需要辅助放疗的患者有资格入组该研究。对照组患者将接受乳房或胸壁放疗(伴/不伴区域淋巴结),剂量为 40Gy/15 个疗程/3 周,而实验组患者将接受 26Gy/5 个疗程/1 周(同一体积)的放疗。对于接受保乳治疗的患者,可以使用同步整合加量放疗(剂量分别为 8Gy 和 6Gy)。假设对照组 5 年局部区域复发率为 5%(对应风险比为 1.63),则 2100 例患者的样本量有 80%的把握力检测出 5 年局部区域复发率 3%的非劣效性,单侧Ⅰ类错误率为 2.5%。患者将在 5 年内招募,并在随后的 5 年内进行随访。
如果证明乳腺癌 5 个疗程的方案不劣效,这将显著改善放疗的可及性,并降低治疗成本。该试验同时为全国范围内的放疗实践标准化和质量保证提供了机会。结合 FAST-Forward 试验的结果,将确定该干预措施在需要区域淋巴结放疗的晚期淋巴结阳性疾病中的安全性。
该试验已在印度临床试验注册中心(CTRI)注册,注册号:CTRI/2018/12/016816(2018 年 12 月 31 日),并在 ClinicalTrial.gov 网站注册,注册号:NCT03788213(2018 年 12 月 28 日)。