Handa Kazuma, Fukui Shinya, Kitahara Mutsunori, Kakizawa Yumi, Nishi Hiroyuki
Department of Cardiovascular Surgery, Osaka General Medical Center, 3-1-56 Bandai-Higashi, Sumiyoshi, Osaka, 556-8558, Japan.
Surg Case Rep. 2020 Oct 1;6(1):244. doi: 10.1186/s40792-020-00978-8.
The recent remarkable development of cardiac imaging technology for unroofed coronary sinus syndrome has led to accurate preoperative diagnosis. We report a case of unroofed coronary sinus syndrome repaired via a minimally invasive approach, under the excellent command of three-dimensional transesophageal echocardiography.
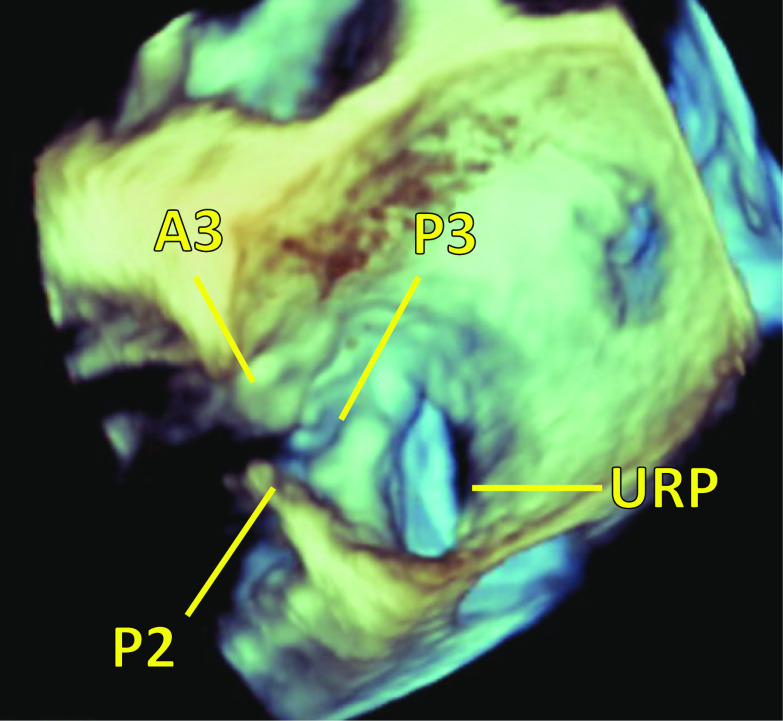
A 77-year-old woman with hypertension was admitted for aggravation of bilateral leg edema and diagnosed with type III unroofed coronary sinus syndrome with Qp/Qs ratio of 1.6:1. The unroofed portion was detected at the atrial side between P2 and P3 of posterior mitral leaflet by preoperative three-dimensional transesophageal echocardiography. Right minithoracotomy was performed at the fourth intercostal space and cardiopulmonary bypass routinely established. Right atriotomy and left atriotomy incisions were made under antegrade cardioplegic arrest. The unroofed portion was revealed at the same location by preoperative transesophageal echocardiography and was clearly recognized only by endoscopy, not by direct vision. It was repaired by direct running suture under endoscopic visualization. We observed no blood cardioplegia leakage or mitral insufficiency, which was also confirmed by postoperative transesophageal echocardiography. The patient's postoperative course was uneventful and she was discharged home 14 days after surgery without any residual shunt.
Successful repair of unroofed coronary sinus syndrome was safely and effectively achieved by a minimally invasive approach supported by preoperative three-dimensional transesophageal echocardiography.
用于无顶冠状静脉窦综合征的心脏成像技术最近取得了显著进展,从而实现了准确的术前诊断。我们报告一例在三维经食管超声心动图的精准引导下,通过微创方法修复无顶冠状静脉窦综合征的病例。
一名77岁高血压女性因双侧腿部水肿加重入院,被诊断为III型无顶冠状静脉窦综合征,Qp/Qs比值为1.6:1。术前三维经食管超声心动图在二尖瓣后叶P2和P3之间的心房侧检测到无顶部分。在第四肋间进行右胸小切口,常规建立体外循环。在顺行性心脏停搏下进行右心房切开和左心房切开切口。术前经食管超声心动图显示无顶部分位于相同位置,仅通过内镜清晰识别,直视下无法看清。在内镜直视下通过连续直接缝合进行修复。我们未观察到心脏停搏液漏血或二尖瓣关闭不全,术后经食管超声心动图也证实了这一点。患者术后恢复顺利,术后14天出院,无任何残余分流。
在术前三维经食管超声心动图的支持下,通过微创方法安全有效地成功修复了无顶冠状静脉窦综合征。