Bajunaid Khalid, Alatar Abdullah, Alqurashi Ashwag, Alkutbi Mohammad, Alzahrani Anas H, Sabbagh Abdulrahman J, Alobaid Abdullah, Barnawi Abdulwahed, Alferayan Ahmed A, Alkhani Ahmed M, Bin Salamah Ali, Sheikh Bassem Y, Alotaibi Fahad E, Alabbas Faisal, Farrash Faisal, Al-Jehani Hosam M, Alhabib Husam, Alnaami Ibrahim, Altweijri Ikhlass, Khoja Isam, Taha Mahmoud, Alzahrani Moajeb, Bafaquh Mohammed S, Binmahfoodh Mohammed, Algahtany Mubarak A, Al-Rashed Sabah, Raza Syed M, Elwatidy Sherif, Alomar Soha A, Al-Issawi Wisam, Khormi Yahya H, Ammar Ahmad, Al-Habib Amro, Baeesa Saleh S, Ajlan Abdulrazag
Department of Surgery, Faculty of Medicine, University of Jeddah, Jeddah, Saudi Arabia; Department of Neurology and Neurosurgery, Montreal Neurological Institute and Hospital, McGill University, Montreal, Quebec, Canada.
Neurosurgery Division, Department of Surgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia.
Clin Neurol Neurosurg. 2020 Nov;198:106237. doi: 10.1016/j.clineuro.2020.106237. Epub 2020 Sep 17.
This observational cross-sectional multicenter study aimed to evaluate the longitudinal impact of the coronavirus disease 2019 (COVID-19) pandemic on neurosurgical practice.
We included 29 participating neurosurgeons in centers from all geographical regions in the Kingdom of Saudi Arabia. The study period, which was between March 5, 2020 and May 20, 2020, was divided into three equal periods to determine the longitudinal effect of COVID-19 measures on neurosurgical practice over time.
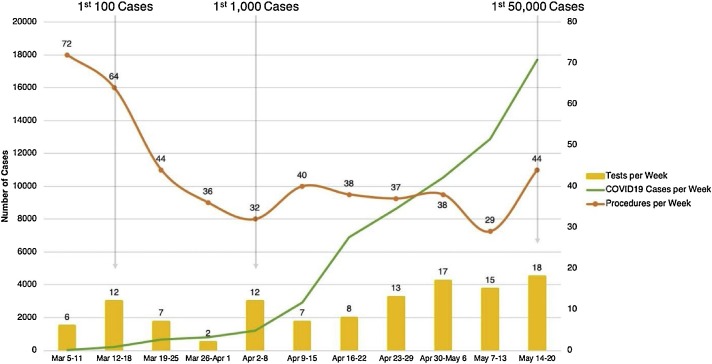
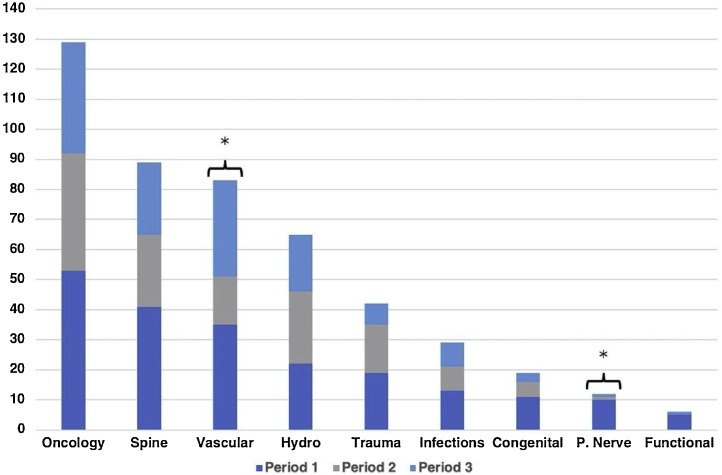
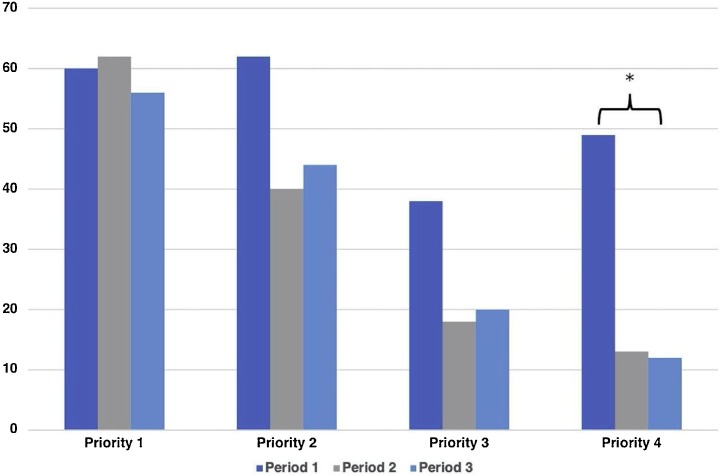
During the 11-week study period, 474 neurosurgical interventions were performed. The median number of neurosurgical procedures per day was 5.5 (interquartile range [IQR]: 3.5-8). The number of cases declined from 72 in the first week and plateaued at the 30's range in subsequent weeks. The most and least number of performed procedures were oncology (129 [27.2 %]) and functional procedures (6 [1.3 %]), respectively. Emergency (Priority 1) cases were more frequent than non-urgent (Priority 4) cases (178 [37.6 %] vs. 74 [15.6 %], respectively). In our series, there were three positive COVID-19 cases. There was a significant among-period difference in the length of hospital stay, which dropped from a median stay of 7 days (IQR: 4-18) to 6 (IQR: 3-13) to 5 days (IQR: 2-8). There was no significant among-period difference with respect to institution type, complications, or mortality.
Our study demonstrated that the COVID-19 pandemic decreased the number of procedures performed in neurosurgery practice. The load of emergency neurosurgery procedures did not change throughout the three periods, which reflects the need to designate ample resources to cover emergencies. Notably, with strict screening for COVID -19 infections, neurosurgical procedures could be safely performed during the early pandemic phase. We recommend to restart performing neurosurgical procedures once the pandemic gets stabilized to avoid possible post pandemic health-care system intolerable overload.
这项观察性横断面多中心研究旨在评估2019年冠状病毒病(COVID-19)大流行对神经外科实践的长期影响。
我们纳入了沙特阿拉伯王国所有地理区域中心的29名参与研究的神经外科医生。研究期间为2020年3月5日至2020年5月20日,分为三个相等的时间段,以确定COVID-19措施随时间对神经外科实践的长期影响。
在为期11周的研究期间,共进行了474例神经外科手术。每天神经外科手术的中位数为5.5(四分位间距[IQR]:3.5 - 8)。病例数从第一周的72例下降,在随后几周稳定在30例左右。手术最多和最少的分别是肿瘤手术(129例[27.2%])和功能性手术(6例[1.3%])。急诊(1级优先)病例比非急诊(4级优先)病例更常见(分别为178例[37.6%]和74例[15.6%])。在我们的系列研究中,有3例COVID-19阳性病例。住院时间存在显著的时间段差异,从中位数住院7天(IQR:4 - 18)降至6天(IQR:3 - 13)再降至5天(IQR:2 - 8)。在机构类型、并发症或死亡率方面,各时间段之间没有显著差异。
我们的研究表明,COVID-19大流行减少了神经外科实践中的手术数量。急诊神经外科手术的负担在三个时间段内没有变化,这反映了需要指定充足资源以应对紧急情况。值得注意的是,通过对COVID - 19感染进行严格筛查,在大流行早期阶段可以安全地进行神经外科手术。我们建议在大流行稳定后重新开始进行神经外科手术,以避免大流行后可能出现的医疗保健系统无法承受的超负荷情况。