Cardiac Surgery, Centre Hospitalier Universitaire Vaudois, Lausanne University, Lausanne, Switzerland.
General Practitioner, Losone, Switzerland.
Eur J Cardiothorac Surg. 2021 Jan 29;59(2):473-478. doi: 10.1093/ejcts/ezaa351.
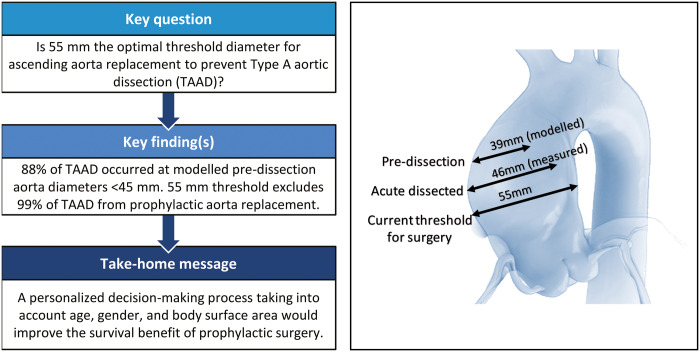
Current guidelines recommend prophylactic replacement of the ascending aorta at an aneurysmal diameter of >55 mm to prevent acute Type A aortic dissection (TAAD) in non-Marfan patients. Several publications have challenged this threshold, suggesting that surgery should be performed in smaller aneurysms to prevent this devastating disease. We reviewed our experience with measuring aortic size at the time of TAAD to validate the existing recommendation for prophylactic ascending aorta replacement.
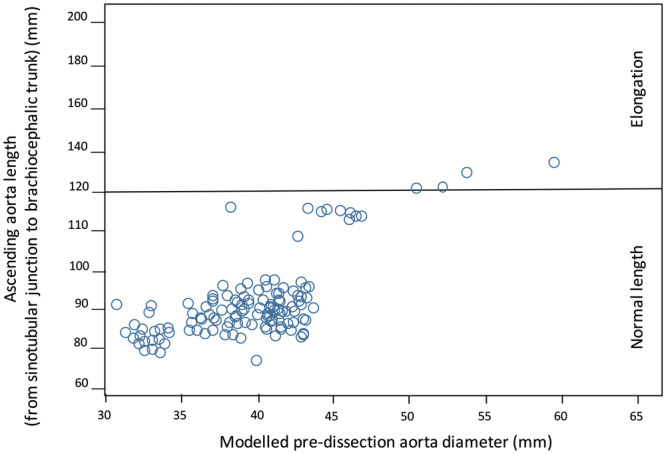
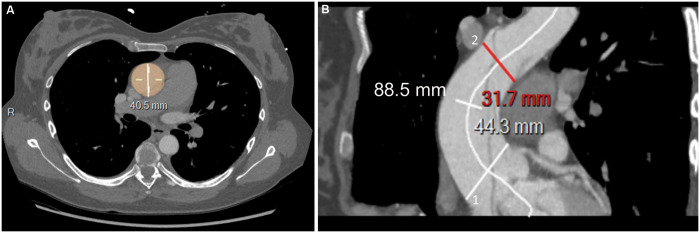
All patients who had been admitted for TAAD to our emergency department from 2014 to 2019 and underwent ascending aorta replacement were included. Marfan patients were excluded. The maximum diameter of the dissected aorta was measured preoperatively using CT scan. We estimated the aortic diameter at the time of dissection to be 7 mm smaller than the measured maximum diameter of the dissected aorta (modelled pre-dissection diameter).
Overall, 102 patients were included. Of these, 67 were male (65.6%) and 35 were female (34.4%), and the cohort's mean age was 65 ± 12.1 years. In addition, 66% were treated for arterial hypertension. The mean maximum modelled pre-dissection diameter was 39.6 ± 4.8 mm: 39.1 ± 5.1 mm in men and 40.7 ± 2.8 mm in women (P = 0.1). The cumulative 30-day mortality rate was 19.6% (20/102).
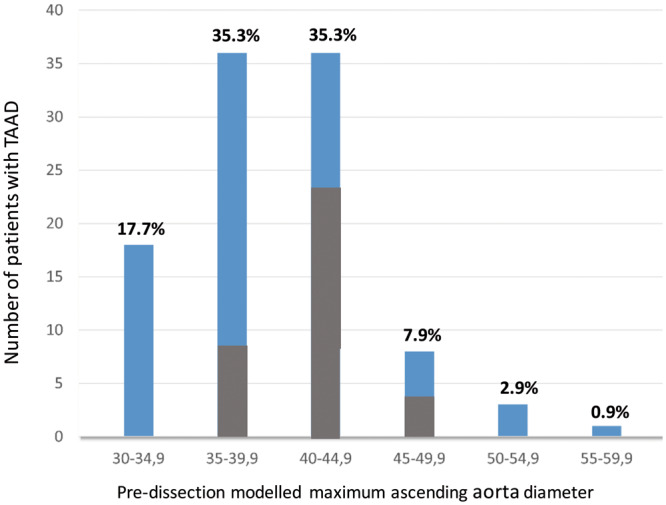
TAAD occurred at a modelled aortic diameter below 45 mm in 87.7% of our patients. Therefore, the current aortic diameter threshold of 55 mm excludes ∼99% of patients with TAAD from prophylactic replacement of the ascending aorta. The maximum diameter of the ascending aorta warrants reappraisal and this parameter should be a distinct part of a personalized decision-making process that also takes into account age, gender and body surface area to establish the surgical indication for preventive aorta replacement aimed to improve the survival benefit of this procedure.
目前的指南建议在非马凡氏综合征患者的升主动脉直径>55mm 时预防性置换升主动脉,以预防急性A型主动脉夹层(TAAD)。一些出版物对这一阈值提出了质疑,认为应在较小的动脉瘤中进行手术,以预防这种破坏性疾病。我们回顾了我们在 TAAD 时测量主动脉大小的经验,以验证预防性升主动脉置换的现有建议。
纳入 2014 年至 2019 年因 TAAD 入住我院急诊科并接受升主动脉置换的所有患者。排除马凡氏综合征患者。术前使用 CT 扫描测量夹层主动脉的最大直径。我们估计夹层时的主动脉直径比测量的夹层主动脉最大直径小 7mm(模拟夹层前直径)。
共纳入 102 例患者,其中男 67 例(65.6%),女 35 例(34.4%),平均年龄 65±12.1 岁。此外,66%的患者患有高血压。平均最大模拟夹层前直径为 39.6±4.8mm:男性为 39.1±5.1mm,女性为 40.7±2.8mm(P=0.1)。30 天死亡率为 19.6%(20/102)。
我们的患者中有 87.7%的患者在模拟主动脉直径小于 45mm 时发生 TAAD。因此,目前 55mm 的升主动脉直径阈值将 99%的 TAAD 患者排除在预防性升主动脉置换之外。升主动脉的最大直径需要重新评估,这个参数应该是个体化决策过程的一个明确部分,该过程还应考虑年龄、性别和体表面积,以确定预防性主动脉置换的手术指征,旨在提高该手术的生存获益。