Center for Personalized Cancer Therapy and Division of Hematology and Oncology, Department of Medicine, UC San Diego Moores Cancer Center, La Jolla, CA, USA.
Division of Hematology and Medical Oncology, Department of Internal Medicine, Seoul National University Boramae Medical Center, Seoul, Republic of Korea.
Nat Commun. 2020 Oct 2;11(1):4965. doi: 10.1038/s41467-020-18613-3.
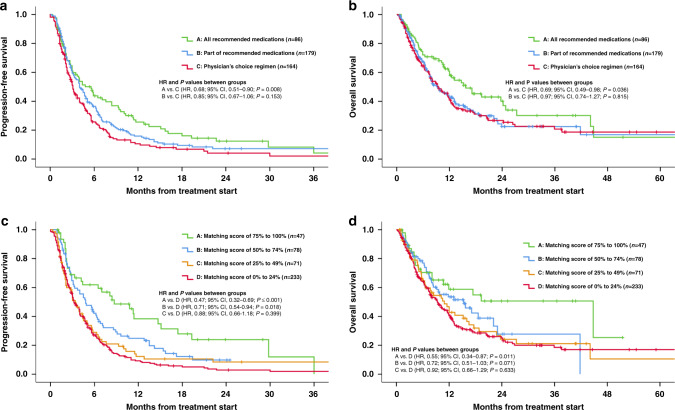
Next-generation sequencing (NGS) can identify novel cancer targets. However, interpreting the molecular findings and accessing drugs/clinical trials is challenging. Furthermore, many tumors show resistance to monotherapies. To implement a precision strategy, we initiated a multidisciplinary (basic/translational/clinical investigators, bioinformaticians, geneticists, and physicians from multiple specialties) molecular tumor board (MTB), which included a project manager to facilitate obtaining clinical-grade biomarkers (blood/tissue NGS, specific immunohistochemistry/RNA expression including for immune-biomarkers, per physician discretion) and medication-acquisition specialists/clinical trial coordinators/navigators to assist with medication access. The MTB comprehensively reviewed patient characteristics to develop N-of-One treatments implemented by the treating physician's direction under the auspices of a master protocol. Overall, 265/429 therapy-evaluable patients (62%) were matched to ≥1 recommended drug. Eighty-six patients (20%) matched to all drugs recommended by MTB, including combinatorial approaches, while 38% received physician's choice regimen, generally with unmatched approach/low degree of matching. Our results show that patients who receive MTB-recommended regimens (versus physician choice) have significantly longer progression-free (PFS) and overall survival (OS), and are better matched to therapy. High (≥50%) versus low (<50%) Matching Score therapy (roughly reflecting therapy matched to ≥50% versus <50% of alterations) independently correlates with longer PFS (hazard ratio [HR], 0.63; 95% confidence interval [CI], 0.50-0.80; P < 0.001) and OS (HR, 0.67; 95% CI, 0.50-0.90; P = 0.007) and higher stable disease ≥6 months/partial/complete remission rate (52.1% versus 30.4% P < 0.001) (all multivariate). In conclusion, patients who receive MTB-based therapy are better matched to their genomic alterations, and the degree of matching is an independent predictor of improved oncologic outcomes including survival.
下一代测序 (NGS) 可鉴定新的癌症靶点。然而,解释分子发现并获得药物/临床试验极具挑战性。此外,许多肿瘤对单药治疗具有抗药性。为了实施精准策略,我们成立了一个多学科(基础/转化/临床研究人员、生物信息学家、遗传学家和来自多个专业的医生)分子肿瘤委员会 (MTB),其中包括一名项目经理,以方便获得临床级别的生物标志物(血液/组织 NGS、特定免疫组化/RNA 表达,包括免疫生物标志物,由医生自行决定)和药物获取专家/临床试验协调员/导航员,以协助获取药物。MTB 全面审查了患者特征,以根据主治医生的方向制定 N-of-One 治疗方案,在主方案的支持下实施。总体而言,265/429 名可评估治疗的患者(62%)与 ≥1 种推荐药物相匹配。86 名患者(20%)与 MTB 推荐的所有药物相匹配,包括联合治疗方法,而 38%的患者接受了医生选择的方案,通常是不匹配的方法/低匹配程度。我们的结果表明,接受 MTB 推荐方案(与医生选择相比)的患者具有更长的无进展生存期 (PFS) 和总生存期 (OS),并且与治疗的匹配度更好。高(≥50%)与低(<50%)匹配评分治疗(大致反映治疗与≥50%与<50%的改变相匹配)与更长的 PFS(风险比 [HR],0.63;95%置信区间 [CI],0.50-0.80;P < 0.001)和 OS(HR,0.67;95% CI,0.50-0.90;P = 0.007)和更高的稳定疾病≥6 个月/部分/完全缓解率(52.1%比 30.4%,P < 0.001)(所有多变量)独立相关。总之,接受基于 MTB 的治疗的患者与他们的基因组改变更匹配,匹配程度是改善包括生存在内的肿瘤学结果的独立预测因素。